

Prevalence, Treatment, and Outcomes of Coexistent Pulmonary Hypertension and Interstitial Lung Disease in Systemic Sclerosis
- PMID: 30762947
- PMCID: PMC6663644
- DOI: 10.1002/art.40862
Prevalence, Treatment, and Outcomes of Coexistent Pulmonary Hypertension and Interstitial Lung Disease in Systemic Sclerosis
Abstract
Objective: Systemic sclerosis (SSc) is associated with interstitial lung disease (ILD) and pulmonary hypertension (PH). This study was undertaken to determine the prevalence, characteristics, treatment, and outcomes of PH in a cohort of patients with SSc-associated ILD.
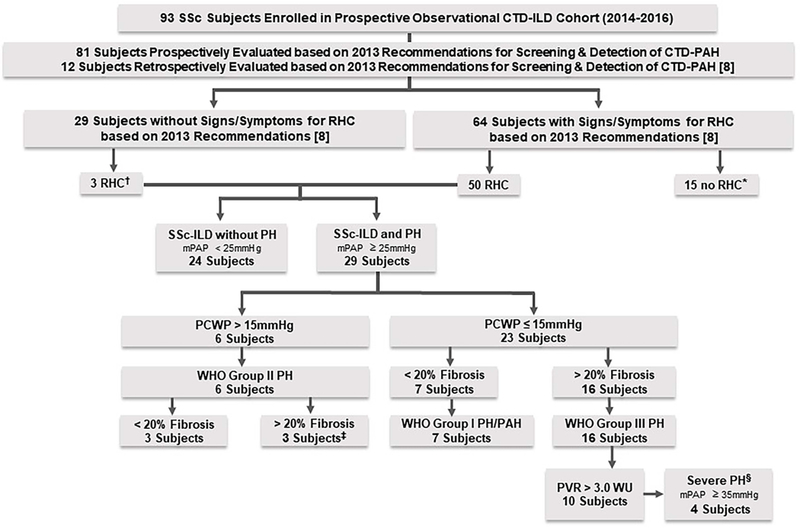
Methods: Patients with SSc-associated ILD on high-resolution computed tomography (HRCT) were included in a prospective observational cohort. Patients were screened for PH based on a standardized screening algorithm and underwent right-sided heart catheterization (RHC) if indicated. PH classification was based on hemodynamic findings and the extent of ILD on HRCT. Summary statistics and survival using the Kaplan-Meier method were calculated.
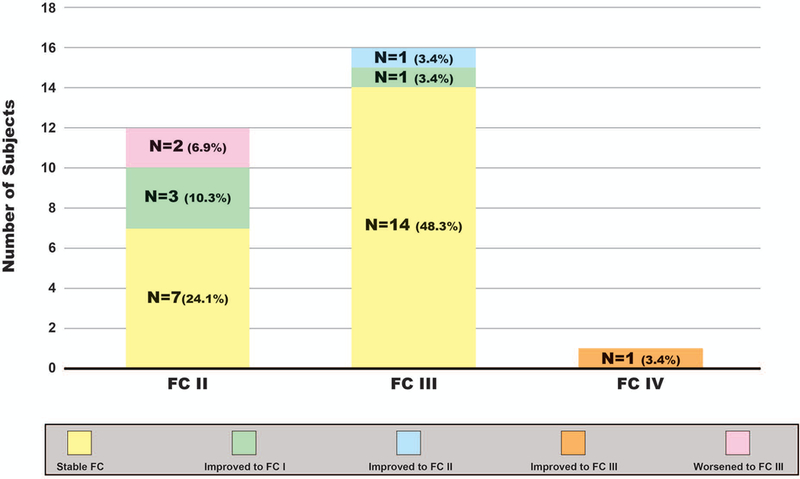
Results: Of the 93 patients with SSc-associated ILD included in the study, 76% were women and 65.6% had diffuse cutaneous SSc. The mean age was 54.9 years, and the mean SSc disease duration was 8 years. Twenty-nine patients (31.2%) had RHC-proven PH; of those 29 patients, 24.1% had PAH, 55.2% had World Health Organization (WHO) Group III PH, 34.5% had WHO Group III PH with pulmonary vascular resistance >3.0 Wood units, 48.3% had a PH diagnosis within 7 years of SSc onset, 82.8% received therapy for ILD, and 82.8% received therapy for PAH. The survival rate 3 years after SSc-associated ILD diagnosis for all patients was 97%. The survival rate 3 years after PH diagnosis for those with SSc-associated ILD and PH was 91%.
Conclusion: In a large cohort of patients with SSc-associated ILD, a significant proportion of patients had coexisting PH, which often occurs early after SSc diagnosis. Most patients were treated with ILD and PAH therapies, and survival was good. Patients with SSc-associated ILD should be evaluated for coexisting PH.
© 2019, American College of Rheumatology.
Conflict of interest statement
Conflict of Interest Disclosures:
Figures
References
-
- Steen VD, Conte C, Owens GR, Medsger TA Jr. Severe restrictive lung disease in systemic sclerosis. Arthritis Rheum 1994;37(9):1283–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
