

Pharmacokinetics of morphine in encephalopathic neonates treated with therapeutic hypothermia
- PMID: 30763356
- PMCID: PMC6375702
- DOI: 10.1371/journal.pone.0211910
Pharmacokinetics of morphine in encephalopathic neonates treated with therapeutic hypothermia
Abstract
Objective: Morphine is a commonly used drug in encephalopathic neonates treated with therapeutic hypothermia after perinatal asphyxia. Pharmacokinetics and optimal dosing of morphine in this population are largely unknown. The objective of this study was to describe pharmacokinetics of morphine and its metabolites morphine-3-glucuronide and morphine-6-glucuronide in encephalopathic neonates treated with therapeutic hypothermia and to develop pharmacokinetics based dosing guidelines for this population.
Study design: Term and near-term encephalopathic neonates treated with therapeutic hypothermia and receiving morphine were included in two multicenter cohort studies between 2008-2010 (SHIVER) and 2010-2014 (PharmaCool). Data were collected during hypothermia and rewarming, including blood samples for quantification of morphine and its metabolites. Parental informed consent was obtained for all participants.
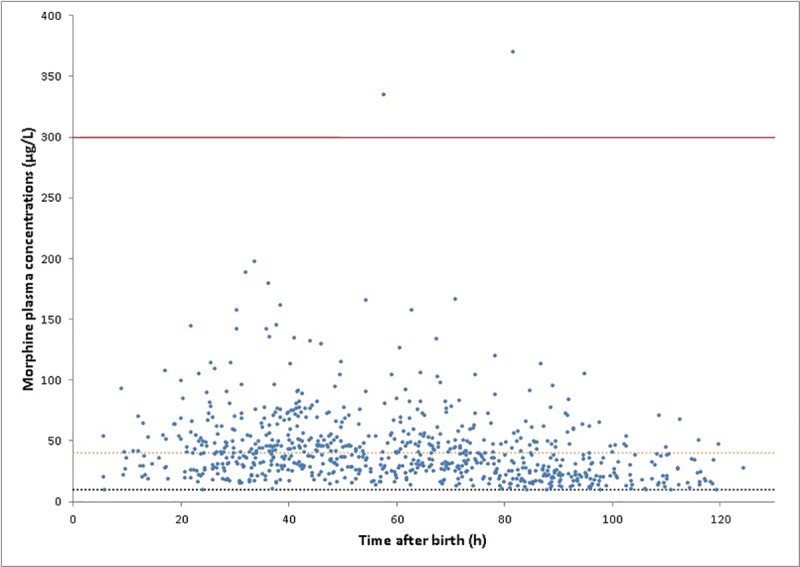
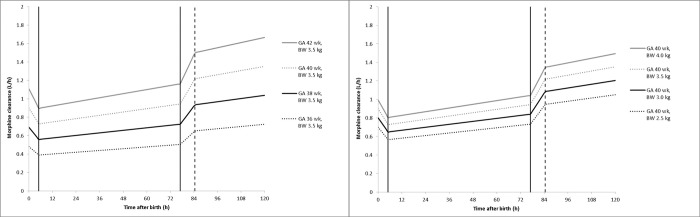
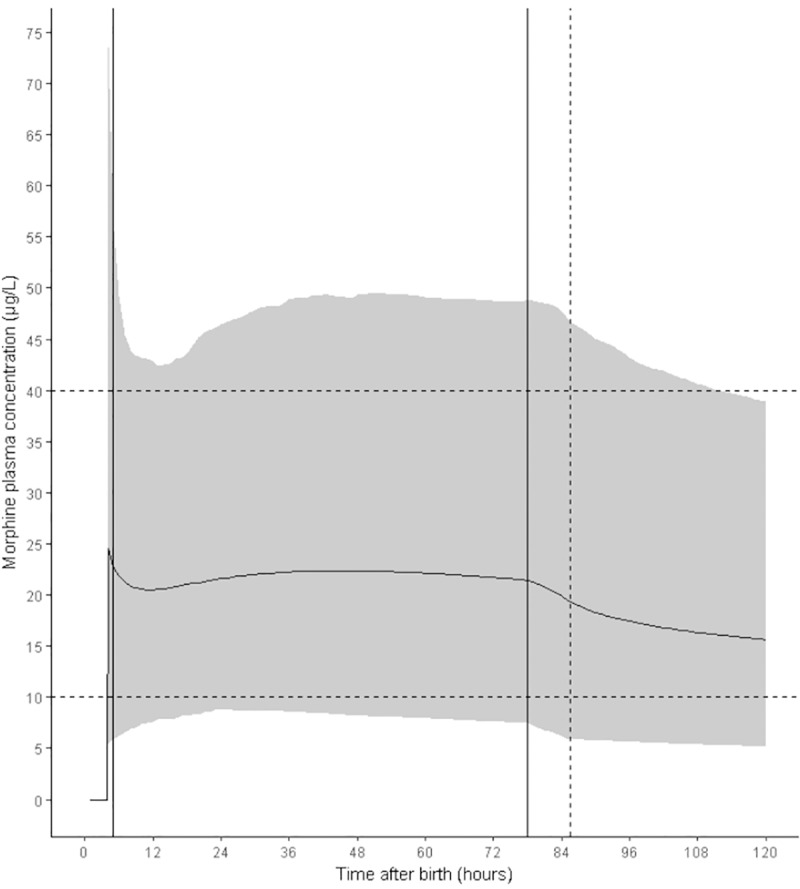
Results: 244 patients (GA mean (sd) 39.8 (1.6) weeks, BW mean (sd) 3,428 (613) g, male 61.5%) were included. Morphine clearance was reduced under hypothermia (33.5°C) by 6.89%/°C (95% CI 5.37%/°C- 8.41%/°C, p<0.001) and metabolite clearance by 4.91%/°C (95% CI 3.53%/°C- 6.22%/°C, p<0.001) compared to normothermia (36.5°C). Simulations showed that a loading dose of 50 μg/kg followed by continuous infusion of 5 μg/kg/h resulted in morphine plasma concentrations in the desired range (between 10 and 40 μg/L) during hypothermia.
Conclusions: Clearance of morphine and its metabolites in neonates is affected by therapeutic hypothermia. The regimen suggested by the simulations will be sufficient in the majority of patients. However, due to the large interpatient variability a higher dose might be necessary in individual patients to achieve the desired effect.
Trial registration: www.trialregister.nl NTR2529.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Groenendaal F, Casaer A, Dijkman KP, Gavilanes AWD, De Haan TR, Ter Horst HJ, et al. Introduction of hypothermia for neonates with perinatal asphyxia in the Netherlands and flanders and the dutch-flemish working group on neonatal neurology. Neonatology. 2013;104: 15–21. 10.1159/000348823 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
