

Therapeutic Options for Neuroendocrine Tumors: A Systematic Review and Network Meta-analysis
- PMID: 30763436
- PMCID: PMC6459123
- DOI: 10.1001/jamaoncol.2018.6720
Therapeutic Options for Neuroendocrine Tumors: A Systematic Review and Network Meta-analysis
Abstract
Importance: Multiple therapies are currently available for patients with neuroendocrine tumors (NETs), yet many therapies have not been compared head-to-head within randomized clinical trials (RCTs).
Objective: To assess the relative safety and efficacy of therapies for NETs.
Data sources: PubMed, Embase, the Cochrane Central Register of Controlled Trials, trial registries, meeting abstracts, and reference lists from January 1, 1947, to March 2, 2018, were searched. Key search terms included neuroendocrine tumors, gastrointestinal neoplasms, therapy, and randomized controlled trial.
Study selection: Randomized clinical trials comparing 2 or more therapies in patients with NETs (primarily gastrointestinal and pancreatic) were evaluated. Thirty RCTs met the selection criteria.
Data extraction and synthesis: Pairs of independent reviewers screened studies, extracted data, and assessed the risk of bias. A network meta-analysis with a frequentist approach was used to compare the efficacy of therapies; the Preferred Reporting Items for Systematic Reviews and Meta-analyses guideline was used.
Main outcomes and measures: Disease control, progression-free survival, overall survival, adverse events, and quality of life.
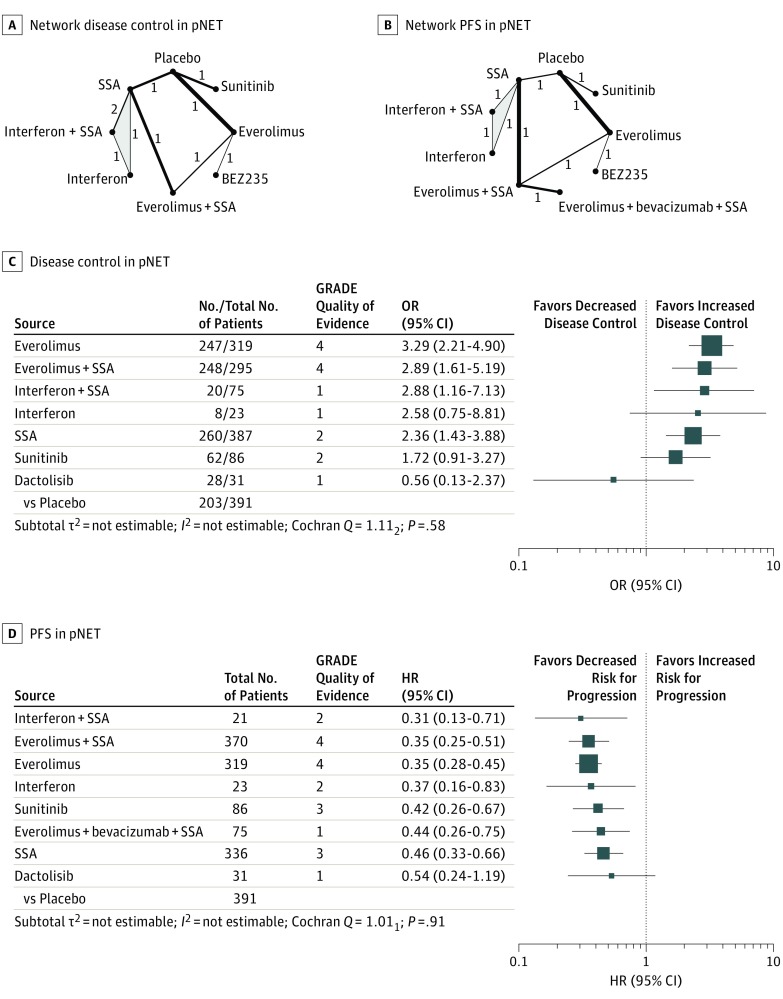
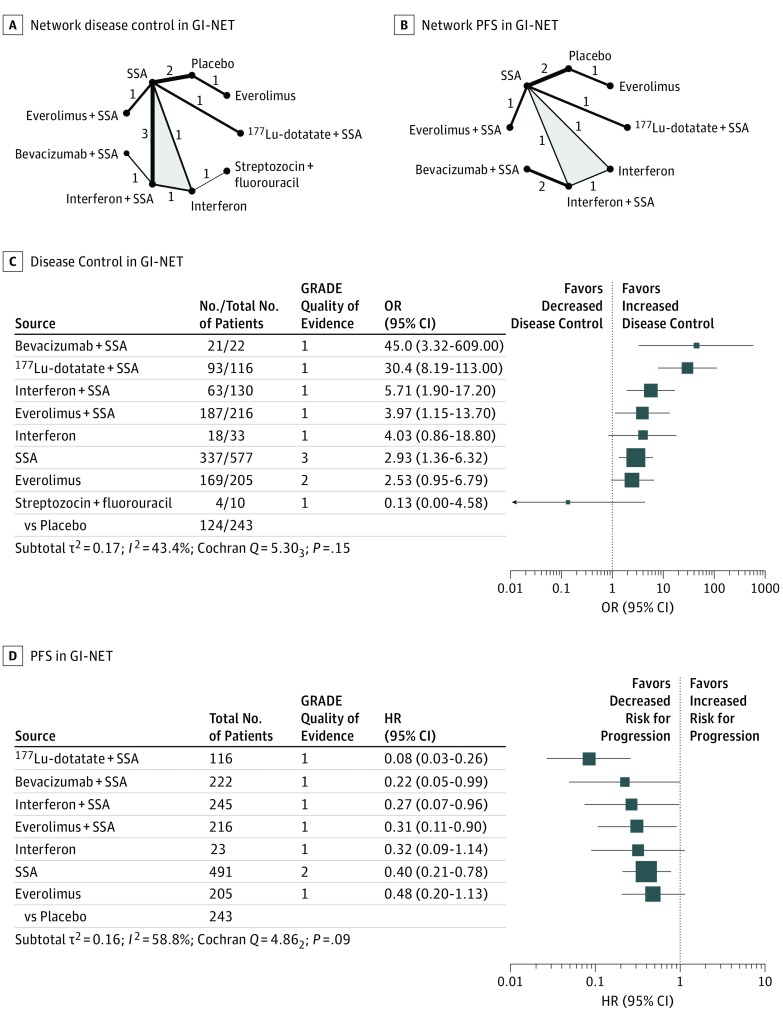
Results: The systematic review identified 30 relevant RCTs comprising 3895 patients (48.4% women) assigned to 22 different therapies for NETs. These therapies showed a broad range of risk for serious and nonserious adverse events. The network meta-analyses included 16 RCTs with predominantly a low risk of bias; nevertheless, precision-of-treatment estimates and estimated heterogeneity were limited. The network meta-analysis found 7 therapies for pancreatic NETs: everolimus (hazard ratio [HR], 0.35 [95% CI, 0.28-0.45]), everolimus plus somatostatin analogue (HR, 0.35 [95% CI, 0.25-0.51]), everolimus plus bevacizumab plus somatostatin analogue (HR, 0.44 [95% CI, 0.26-0.75]), interferon (HR, 0.37 [95% CI, 0.16-0.83]), interferon plus somatostatin analogue (HR, 0.31 [95% CI, 0.13-0.71]), somatostatin analogue (HR, 0.46 [95% CI, 0.33-0.66]), and sunitinib (HR, 0.42 [95% CI, 0.26-0.67]), and 5 therapies for gastrointestinal NETs: bevacizumab plus somatostatin analogue (HR, 0.22 [95% CI, 0.05-0.99]), everolimus plus somatostatin analogue (HR, 0.31 [95% CI, 0.11-0.90]), interferon plus somatostatin analogue (HR, 0.27 [95% CI, 0.07-0.96]), Lu 177-dotatate plus somatostatin analogue (HR, 0.08 [95% CI, 0.03-0.26], and somatostatin analogues (HR, 0.40 [95% CI, 0.21-0.78]) with higher efficacy than placebo and suggests an overall superiority of combination therapies.
Conclusions and relevance: The findings from this study suggest that a range of efficient therapies with different safety profiles is available for patients with NETs.
Conflict of interest statement
Figures
Comment in
-
Evaluating Risks and Benefits of Evolving Systemic Treatments of Neuroendocrine Tumors.JAMA Oncol. 2019 Apr 1;5(4):489-490. doi: 10.1001/jamaoncol.2018.6694. JAMA Oncol. 2019. PMID: 30763444 No abstract available.
References
-
- Yao JC, Fazio N, Singh S, et al. ; RAD001 in Advanced Neuroendocrine Tumours, Fourth Trial (RADIANT-4) Study Group . Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study. Lancet. 2016;387(10022):968-977. doi:10.1016/S0140-6736(15)00817-X - DOI - PMC - PubMed
-
- Yao JC, Guthrie KA, Moran C, et al. . Phase III prospective randomized comparison trial of depot octreotide plus interferon alfa-2b versus depot octreotide plus bevacizumab in patients with advanced carcinoid tumors: SWOG S0518. J Clin Oncol. 2017;35(15):1695-1703. doi:10.1200/JCO.2016.70.4072 - DOI - PMC - PubMed
-
- Strosberg JR, Wolin EM, Chasen B, et al. . NETTER-1 phase III: Progression-free survival, radiographic response, and preliminary overall survival results in patients with midgut neuroendocrine tumors treated with 177-Lu-dotatate. J Clin Oncol. 2016;34(4)(suppl):194-194. doi:10.1200/jco.2016.34.4_suppl.194 - DOI - PubMed
-
- Pavel ME, Hainsworth JD, Baudin E, et al. ; RADIANT-2 Study Group . Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): a randomised, placebo-controlled, phase 3 study. Lancet. 2011;378(9808):2005-2012. doi:10.1016/S0140-6736(11)61742-X - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
