

DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses
- PMID: 30764511
- PMCID: PMC6413235
- DOI: 10.3390/nu11020338
DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses
Abstract
Background: The Dietary Approaches to Stop Hypertension (DASH) dietary pattern, which emphasizes fruit, vegetables, fat-free/low-fat dairy, whole grains, nuts and legumes, and limits saturated fat, cholesterol, red and processed meats, sweets, added sugars, salt and sugar-sweetened beverages, is widely recommended by international diabetes and heart association guidelines.
Objective: To summarize the available evidence for the update of the European Association of the Study of Diabetes (EASD) guidelines, we conducted an umbrella review of existing systematic reviews and meta-analyses using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach of the relation of the DASH dietary pattern with cardiovascular disease and other cardiometabolic outcomes in prospective cohort studies and its effect on blood pressure and other cardiometabolic risk factors in controlled trials in individuals with and without diabetes.
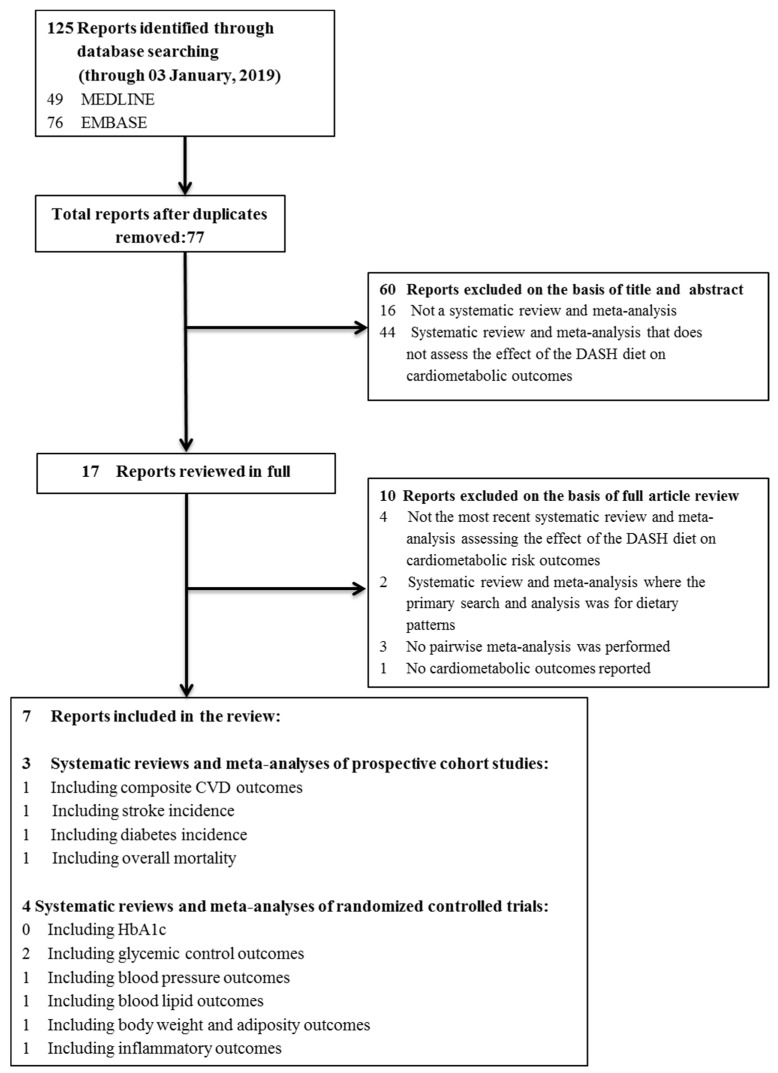
Methods: MEDLINE and EMBASE were searched through 3 January 2019. We included systematic reviews and meta-analyses assessing the relation of the DASH dietary pattern with cardiometabolic disease outcomes in prospective cohort studies and the effect on cardiometabolic risk factors in randomized and non-randomized controlled trials. Two independent reviewers extracted relevant data and assessed the risk of bias of individual studies. The primary outcome was incident cardiovascular disease (CVD) in the prospective cohort studies and systolic blood pressure in the controlled trials. Secondary outcomes included incident coronary heart disease, stroke, and diabetes in prospective cohort studies and other established cardiometabolic risk factors in controlled trials. If the search did not identify an existing systematic review and meta-analysis on a pre-specified outcome, then we conducted our own systematic review and meta-analysis. The evidence was summarized as risk ratios (RR) for disease incidence outcomes and mean differences (MDs) for risk factor outcomes with 95% confidence intervals (95% CIs). The certainty of the evidence was assessed using GRADE.
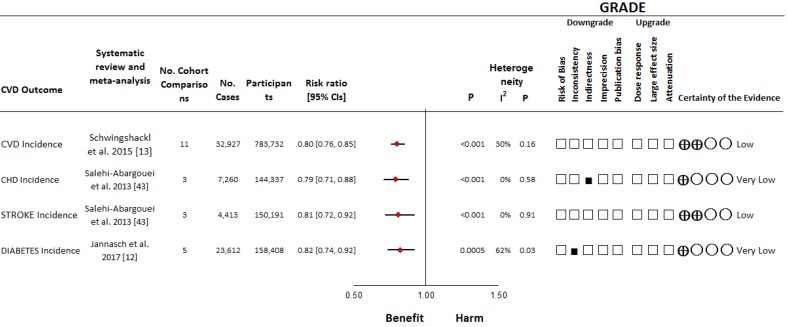
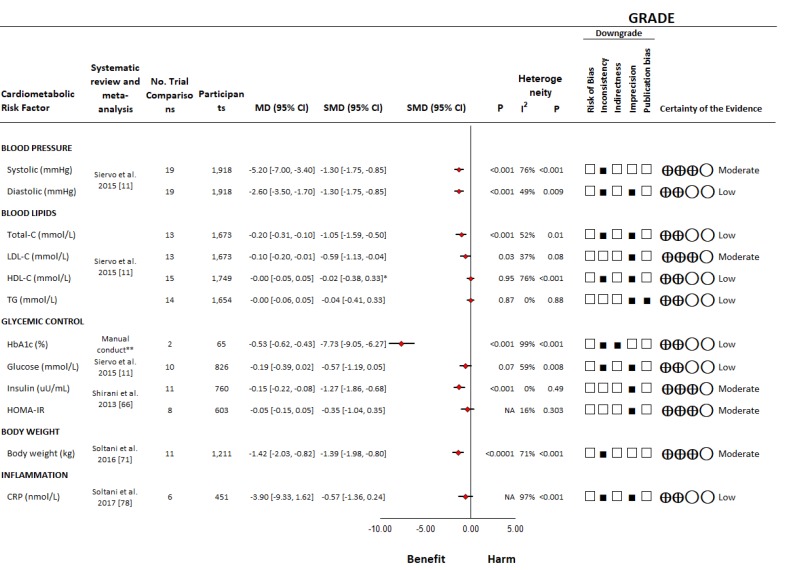
Results: We identified three systematic reviews and meta-analyses of 15 unique prospective cohort studies (n = 942,140) and four systematic reviews and meta-analyses of 31 unique controlled trials (n = 4,414) across outcomes. We conducted our own systematic review and meta-analysis of 2 controlled trials (n = 65) for HbA1c. The DASH dietary pattern was associated with decreased incident cardiovascular disease (RR, 0.80 (0.76⁻0.85)), coronary heart disease (0.79 (0.71⁻0.88)), stroke (0.81 (0.72⁻0.92)), and diabetes (0.82 (0.74⁻0.92)) in prospective cohort studies and decreased systolic (MD, -5.2 mmHg (95% CI, -7.0 to -3.4)) and diastolic (-2.60 mmHg (-3.50 to -1.70)) blood pressure, Total-C (-0.20 mmol/L (-0.31 to -0.10)), LDL-C (-0.10 mmol/L (-0.20 to -0.01)), HbA1c (-0.53% (-0.62, -0.43)), fasting blood insulin (-0.15 μU/mL (-0.22 to -0.08)), and body weight (-1.42 kg (-2.03 to -0.82)) in controlled trials. There was no effect on HDL-C, triglycerides, fasting blood glucose, HOMA-IR, or CRP. The certainty of the evidence was moderate for SBP and low for CVD incidence and ranged from very low to moderate for the secondary outcomes.
Conclusions: Current evidence allows for the conclusion that the DASH dietary pattern is associated with decreased incidence of cardiovascular disease and improves blood pressure with evidence of other cardiometabolic advantages in people with and without diabetes. More research is needed to improve the certainty of the estimates.
Keywords: DASH; GRADE; cardiometabolic health; cardiovascular disease; dietary approaches to stop hypertension; review.
Conflict of interest statement
D.R. has served as principal investigator or co-investigator in clinical trials of AstraZeneca, Eli Lilly, MSD, Novo Nordisk, Sanofi Aventis, Solvay and Trophos. He received honoraria for speaking or advisory board engagements and consulting fees from Abbott, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Lifescan–Johnson and Johnson, Novartis, Novo Nordisk, MSD, Merck Sharp and Dohme, Pfizer, Pliva, Roche, Salvus, Sanofi Aventis and Takeda. He served as a Board member and Secretary of IDF Europe in biennium 2015–2017. He is a president of Croatian Society for Diabetes and Metabolic Disorders of Croatian Medical Association, chair of IDF Young Leaders in Diabetes Programme, Executive committee member of Diabetes and Cardiovascular Disease Study Group of EASD, Croatian Endocrine Society, Croatian Society for Obesity and Croatian Society for Endocrine Oncology. J.S.S. reports serving on the board of and receiving grant support through his institution from the International Nut and Dried Fruit Council, and Eroski Foundation and serving on the Executive Committee of the Instituto Danone Spain and on the Scientific Committee of the Danone International Institute. Has received research support from the Instituto de Salud Carlos III, Spain; Ministerio de Educación y Ciencia, Spain; Departament de Salut Pública de la Generalitat de Catalunya, Catalonia, Spain; European Commission. He has received research support from California Walnut Commission, Sacramento CA, USA; Patrimonio Comunal Olivarero, Spain; La Morella Nuts, Spain; and Borges S.A., Spain. Reports receiving consulting fees or travel expenses from Danone; California Walnut Commission, Eroski Foundation, Instituto Danone–Spain, Nuts for Life, Australian Nut Industry Council, Nestlé, Abbot Laboratories, and Font Vella Lanjarón. He is on the Clinical Practice Guidelines Expert Committee of the European Association for the study of Diabetes (EASD), and served in the Scientific Committee of the Spanish Food and Safety Agency, and the Spanish Federation of the Scientific Societies of Food, Nutrition and Dietetics. He is a member of the International Carbohydrate Quality Consortium (ICQC), and Executive Board Member of the Diabetes and Nutrition Study Group (DNSG) of the EASD. C.W.C.K. has received grant grants or research support from the Advanced Food Materials Network, Agriculture and Agri-Foods Canada (AAFC), Almond Board of California, American Pistachio Growers, Barilla, California Strawberry Commission, Calorie Control Council, Canadian Institutes of Health Research (CIHR), Canola Council of Canada, International Nut and Dried Fruit Council, International Tree Nut Council Research and Education Foundation, Loblaw Brands Ltd., Pulse Canada, Saskatchewan Pulse Growers and Unilever. He has received in-kind research support from the Almond Board of California, California Walnut Council, American Peanut Council, Barilla, Unilever, Unico/Primo, Loblaw Companies, Quaker (Pepsico), Pristine Gourmet, Kellogg Canada, WhiteWave Foods. He has received travel support and/or honoraria from the American Peanut Council, American Pistachio Growers, Barilla, Bayer, California Walnut Commission, Canola Council of Canada, General Mills, International Tree Nut Council, Loblaw Brands Ltd., Nutrition Foundation of Italy, Oldways Preservation Trust, Orafti, Paramount Farms, Peanut Institute, Pulse Canada, Sabra Dipping Co., Saskatchewan Pulse Growers, Sun-Maid, Tate and Lyle, Unilever and White Wave Foods. He has served on the scientific advisory board for the International Tree Nut Council, McCormick Science Institute, Oldways Preservation Trust, Paramount Farms and Pulse Canada. He is a member of the International Carbohydrate Quality Consortium (ICQC), Executive Board Member of the Diabetes and Nutrition Study Group (DNSG) of the European Association for the Study of Diabetes (EASD), is on the Clinical Practice Guidelines Expert Committee for Nutrition Therapy of the EASD and is a Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation. J.L.S. has received research support from the Canadian Institutes of health Research (CIHR), Diabetes Canada, PSI Foundation, Banting and Best Diabetes Centre (BBDC), Canadian Nutrition Society (CNS), American Society for Nutrition (ASN), INC International Nut and Dried Fruit Council Foundation, National Dried Fruit Trade Association, The Tate and Lyle Nutritional Research Fund at the University of Toronto, The Glycemic Control and Cardiovascular Disease in Type 2 Diabetes Fund at the University of Toronto (a fund established by the Alberta Pulse Growers) and the Nutrition Trialists Fund at the University of Toronto (a fund established by the Calorie Control Council). He has received in-kind research support from the Almond Board of California, California Walnut Commission, American Peanut Council, Barilla, Unilever, Unico/Primo, Loblaw Companies, Quaker (Pepsico), Kellogg Canada, WhiteWave Foods. He has received travel support, speaker fees and/or honoraria from Diabetes Canada, Canadian Nutrition Society (CNS), Mott’s LLP, Dairy Farmers of Canada, FoodMinds LLC, Memac Ogilvy & Mather LLC, PepsiCo, The Ginger Network LLC, International Sweeteners Association, Nestlé, Pulse Canada, Canadian Society for Endocrinology and Metabolism (CSEM), GI Foundation, Abbott, Biofortis, American Society for Nutrition (ASN), and Physicians Committee for Responsible Medicine. He has ad hoc consulting arrangements with Perkins Coie LLP, Tate and Lyle, and Wirtschaftliche Vereinigung Zucker e.V. He is a member of the European Fruit Juice Association Scientific Expert Panel. He is on the Clinical Practice Guidelines Expert Committees of Diabetes Canada, European Association for the study of Diabetes (EASD), Canadian Cardiovascular Society (CCS), and Obesity Canada. He serves as an unpaid scientific advisor for the Food, Nutrition, and Safety Program (FNSP) and the Technical Committee on Carbohydrates of the International Life Science Institute (ILSI) North America. He is a member of the International Carbohydrate Quality Consortium (ICQC), Executive Board Member of the Diabetes and Nutrition Study Group (DNSG) of the EASD, and Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation. No competing interests were declared by L.C., E.V., S.K.N., S.B.M., and H.K.
Figures
References
-
- International Diabetes Federation IDF Diabetes Atlas. [(accessed on 30 January 2018)];2015 Available online: http://www.diabetesatlas.org/resources/2015-atlas.html.
-
- O’Rourke K., VanderZanden A., Shepard D., Leach-Kemon K. Cardiovascular disease worldwide, 1990–2013. JAMA. 2015;314:1905. doi: 10.1001/jama.2015.14994. - DOI
-
- World Health Organization (WHO) Obesity. [(accessed on 30 January 2018)]; Available online: http://www.who.int/gho/ncd/riskfactors/obesity_text/en/
-
- Chobanian A.V., Bakris G.L., Black H.R., Cushman W.C., Green L.A., Izzo J.L., Jr., Jones D.W., Materson B.J., Oparil S., Wright J.T., Jr., et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA. 2003;289:2560–2572. doi: 10.1001/jama.289.19.2560. - DOI - PubMed
-
- American Heart Association Nutrition Committee. Lichtenstein A.H., Appel L.J., Brands M., Carnethon M., Daniels S., Franch H.A., Franklin B., Kris-Etherton P., Harris W.S., et al. Diet and lifestyle recommendations revision 2006: A scientific statement from the American Heart Association Nutrition Committee. Circulation. 2006;114:82–96. doi: 10.1161/CIRCULATIONAHA.106.176158. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
