

Interventions to Promote Patient Utilization of Cardiac Rehabilitation: Cochrane Systematic Review and Meta-Analysis
- PMID: 30764517
- PMCID: PMC6406265
- DOI: 10.3390/jcm8020189
Interventions to Promote Patient Utilization of Cardiac Rehabilitation: Cochrane Systematic Review and Meta-Analysis
Abstract
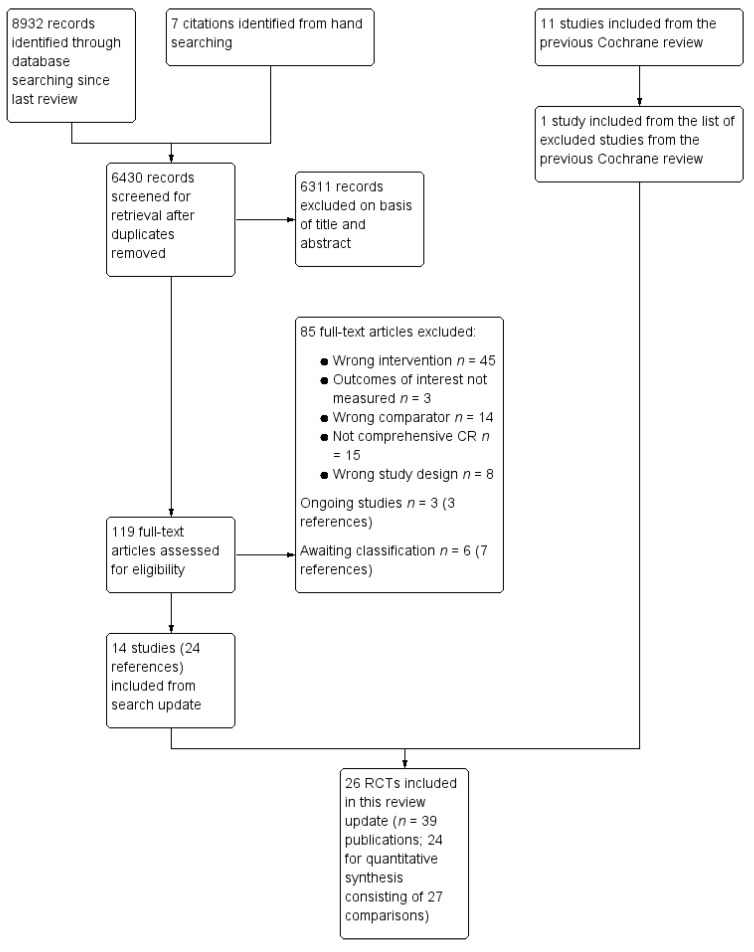
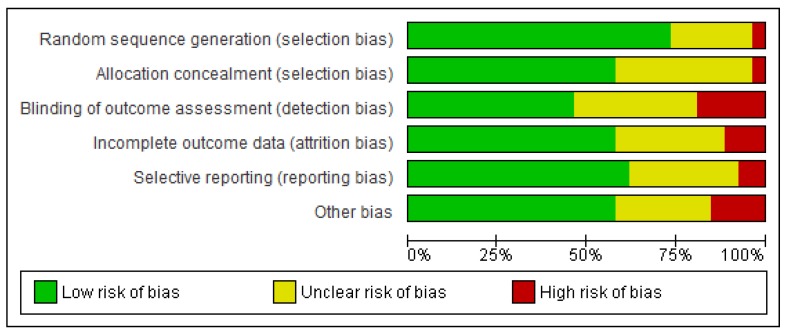
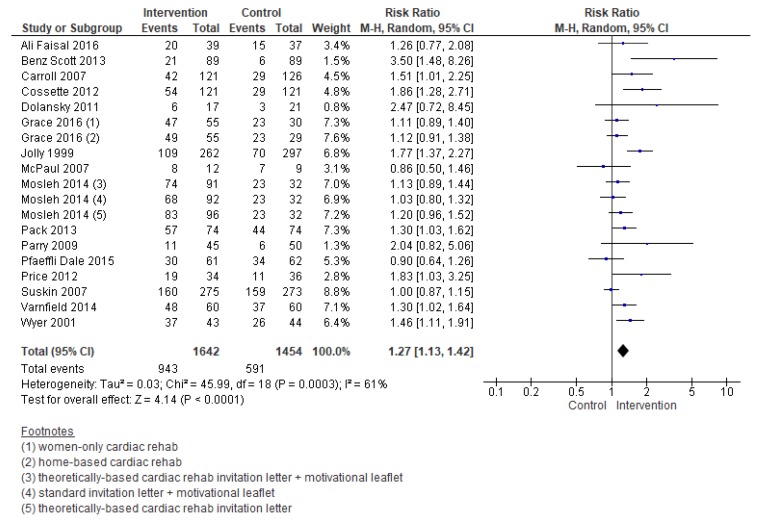
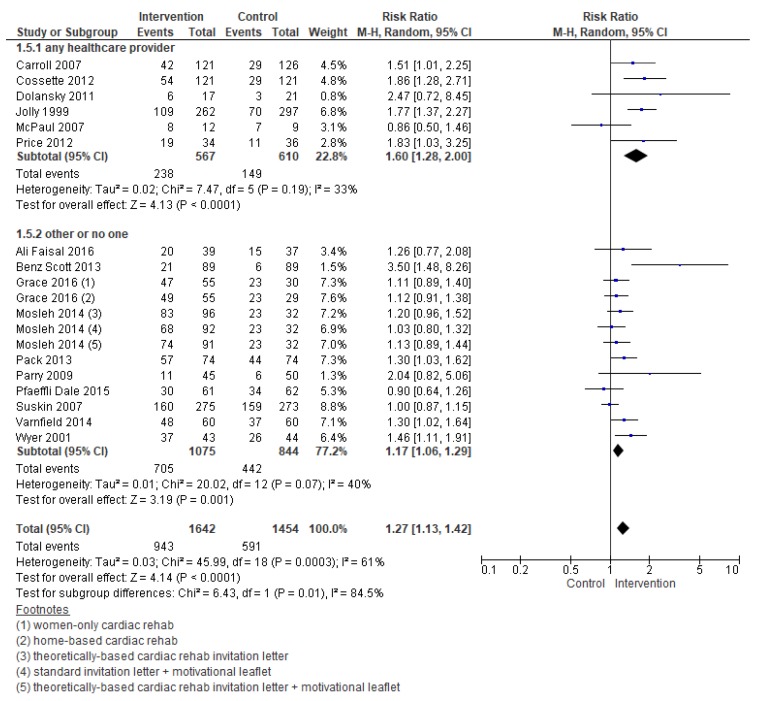
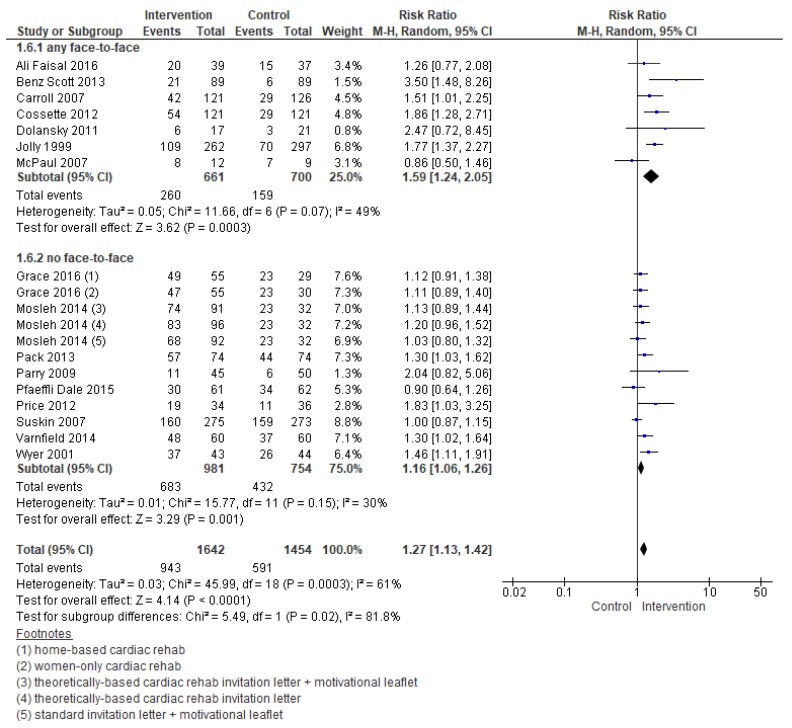
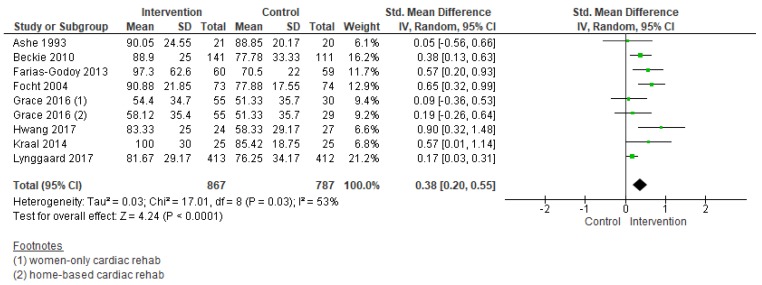
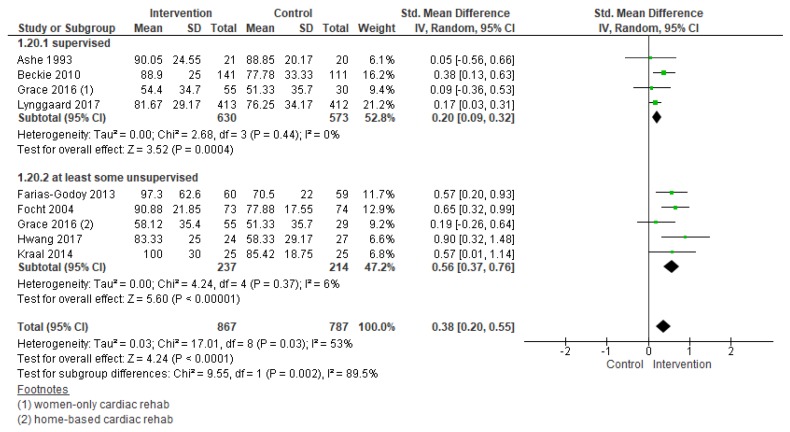
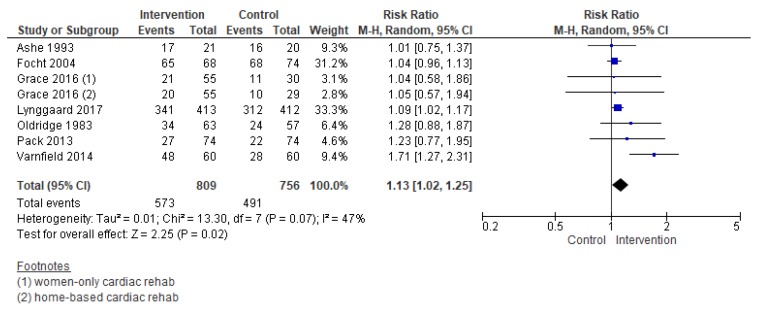
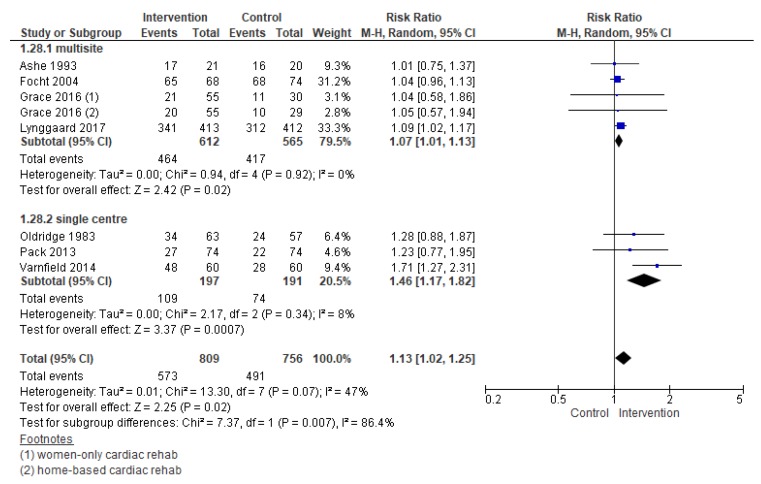
Too few patients utilize cardiac rehabilitation (CR), despite its benefits. The Cochrane review assessing the effectiveness of interventions to increase CR utilization (enrolment, adherence, and completion) was updated. A search was performed through July 2018 of the Cochrane and MEDLINE (Medical Literature Analysis and Retrieval System Online) databases, among other sources. Randomized controlled trials in adults with myocardial infarction, angina, revascularization, or heart failure were included. Interventions had to aim to increase utilization of comprehensive phase II CR. Two authors independently performed all stages of citation processing. Following the random-effects meta-analysis, meta-regression was undertaken to explore the impact of pre-specified factors. Twenty-six trials with 5299 participants were included (35.8% women). Low-quality evidence showed an effect of interventions in increasing enrolment (risk ratio (RR) = 1.27, 95% confidence interval (CI) = 1.13⁻1.42). Meta-regression analyses suggested that the intervention deliverer (nurse or allied healthcare provider, p = 0.02) and delivery format (face-to-face, p = 0.01) were influential in increasing enrolment. There was low-quality evidence that interventions to increase adherence were effective (standardized mean difference (SMD) = 0.38, 95% CI = 0.20⁻0.55), particularly where remotely-offered (SMD = 0.56, 95% CI = 0.36⁻0.76). There was moderate-quality evidence that interventions to increase program completion were effective (RR = 1.13, 95% CI = 1.02⁻1.25). There are effective interventions to increase CR utilization, but more research is needed to establish specific, implementable materials and protocols, particularly for completion.
Keywords: cardiac rehabilitation; coronary artery disease; healthcare access; secondary prevention.
Conflict of interest statement
CSAP: none known. G.C.: none known. P.D.: none known. R.T.: currently a co-author of several other Cochrane Reviews on cardiac rehabilitation. He is Chief Investigator in receipt of ongoing National Institute of Health Research Programme Grants for Applied Research (RP-PG-1210-12004): Rehabilitation Enablement in Chronic Heart Failure (REACH-HF). He was involved in some of the included trials but, was not involved in the RoB or GRADE assessment related to these studies. S.G.: Was principal investigator of an included trial, but did not do the RoB or GRADE assessment relating to the trial.
Figures
References
-
- Benjamin E.J., Virani S.S., Callaway C.W., Chamberlain A.M., Chang A.R., Cheng S., Chiuve S.E., Cushman M., Delling F.N., Deo R., et al. Heart Disease and Stroke Statistics—2018 Update: A Report From the American Heart Association. Circulation. 2018;137:e67–e492. doi: 10.1161/CIR.0000000000000558. - DOI - PubMed
-
- Grace S.L., Turk-Adawi K.I., Contractor A., Atrey A., Campbell N.R.C., Derman W., Ghisi G.L.M., Sarkar B.K., Yeo T.J.T.J., Lopez-Jimenez F., et al. Cardiac Rehabilitation Delivery Model for Low-Resource Settings: An International Council of Cardiovascular Prevention and Rehabilitation consensus statement. Prog. Cardiovasc. Dis. 2016;59:1–20. doi: 10.1016/j.pcad.2016.08.004. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
