

Symptom Subtypes of Obstructive Sleep Apnea Predict Incidence of Cardiovascular Outcomes
- PMID: 30764637
- PMCID: PMC6701040
- DOI: 10.1164/rccm.201808-1509OC
Symptom Subtypes of Obstructive Sleep Apnea Predict Incidence of Cardiovascular Outcomes
Abstract
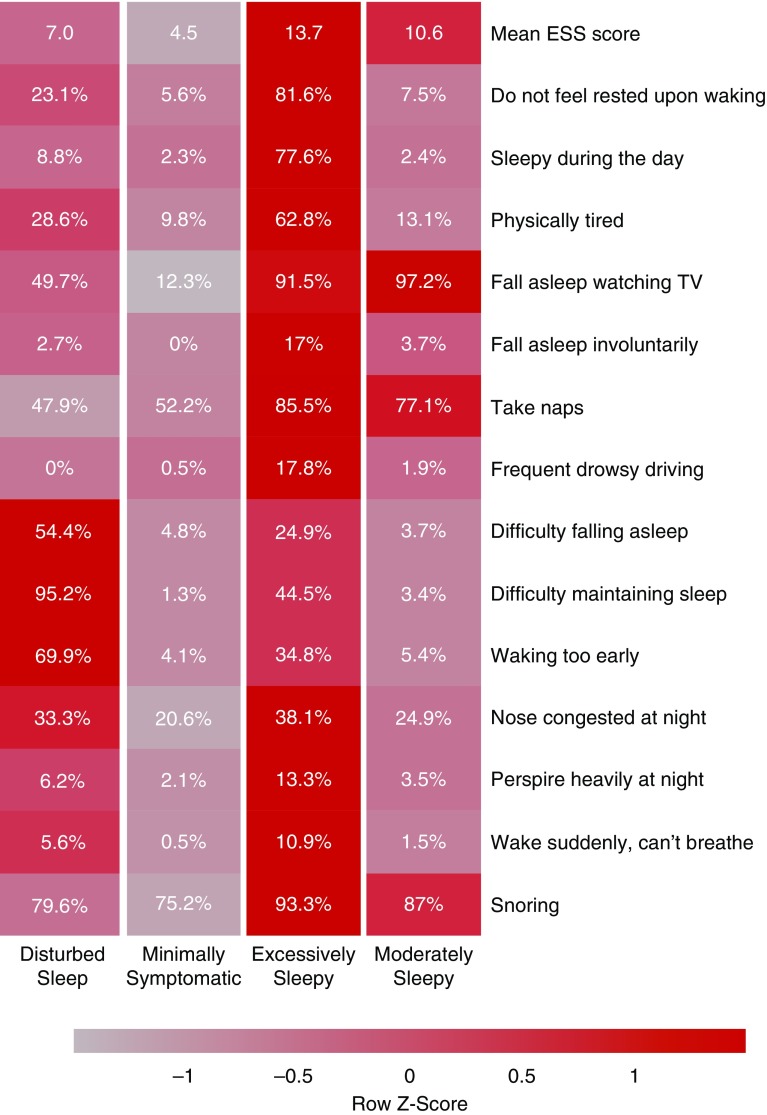
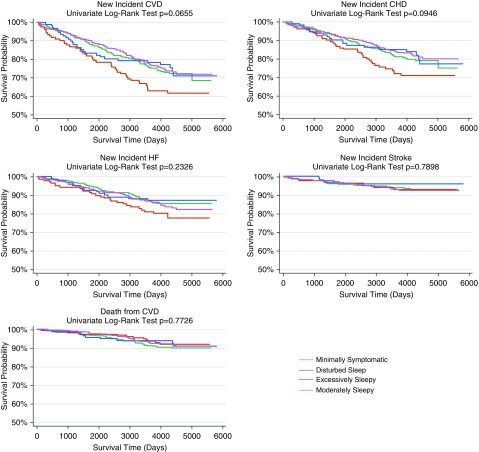
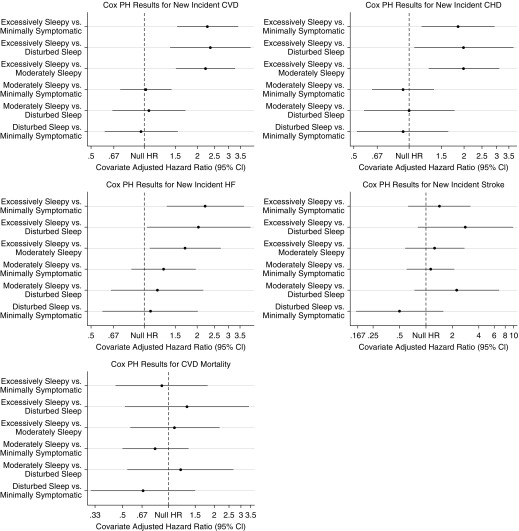
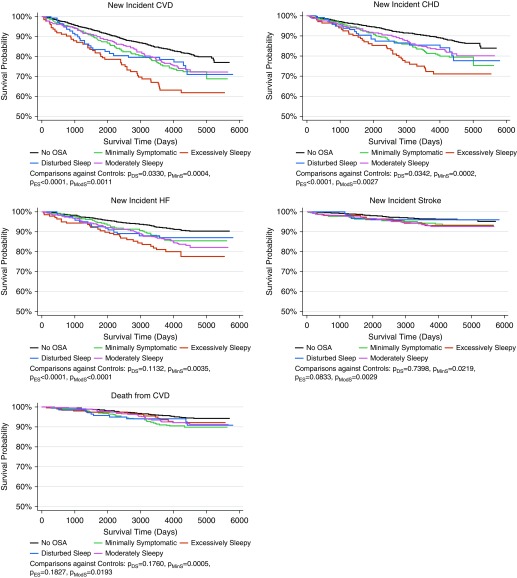
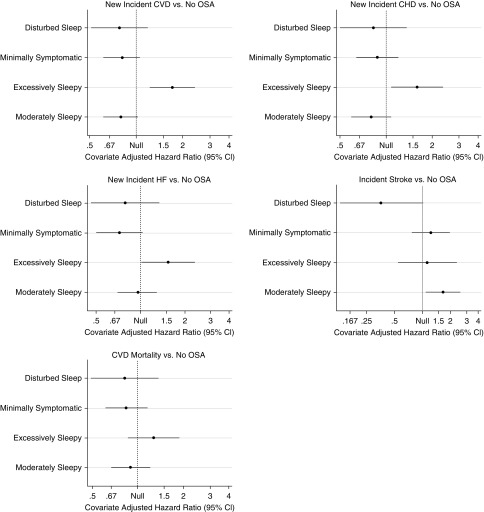
Rationale: Symptom subtypes have been described in clinical and population samples of patients with obstructive sleep apnea (OSA). It is unclear whether these subtypes have different cardiovascular consequences.Objectives: To characterize OSA symptom subtypes and assess their association with prevalent and incident cardiovascular disease in the Sleep Heart Health Study.Methods: Data from 1,207 patients with OSA (apnea-hypopnea index ≥ 15 events/h) were used to evaluate the existence of symptom subtypes using latent class analysis. Associations between subtypes and prevalence of overall cardiovascular disease and its components (coronary heart disease, heart failure, and stroke) were assessed using logistic regression. Kaplan-Meier survival analysis and Cox proportional hazards models were used to evaluate whether subtypes were associated with incident events, including cardiovascular mortality.Measurements and Main Results: Four symptom subtypes were identified (disturbed sleep [12.2%], minimally symptomatic [32.6%], excessively sleepy [16.7%], and moderately sleepy [38.5%]), similar to prior studies. In adjusted models, although no significant associations with prevalent cardiovascular disease were found, the excessively sleepy subtype was associated with more than threefold increased risk of prevalent heart failure compared with each of the other subtypes. Symptom subtype was also associated with incident cardiovascular disease (P < 0.001), coronary heart disease (P = 0.015), and heart failure (P = 0.018), with the excessively sleepy again demonstrating increased risk (hazard ratios, 1.7-2.4) compared with other subtypes. When compared with individuals without OSA (apnea-hypopnea index < 5), significantly increased risk for prevalent and incident cardiovascular events was observed mostly for patients in the excessively sleepy subtype.Conclusions: OSA symptom subtypes are reproducible and associated with cardiovascular risk, providing important evidence of their clinical relevance.
Keywords: cardiovascular disease; cluster analysis; sleep apnea; sleepiness; symptom subtypes.
Figures
Comment in
-
Sleep Apnea Heterogeneity, Phenotypes, and Cardiovascular Risk. Implications for Trial Design and Precision Sleep Medicine.Am J Respir Crit Care Med. 2019 Aug 15;200(4):412-413. doi: 10.1164/rccm.201903-0545ED. Am J Respir Crit Care Med. 2019. PMID: 30916985 Free PMC article. No abstract available.
References
-
- Lim DC, Pack AI. Obstructive sleep apnea: update and future. Annu Rev Med. 2017;68:99–112. - PubMed
-
- American Academy of Sleep Medicine. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The report of an American Academy of Sleep Medicine Task Force. Sleep. 1999;22:667–689. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
