

Benefits of Sequentially Adding Cognitive-Behavioral Therapy or Antidepressant Medication for Adults With Nonremitting Depression
- PMID: 30764648
- PMCID: PMC6557125
- DOI: 10.1176/appi.ajp.2018.18091075
Benefits of Sequentially Adding Cognitive-Behavioral Therapy or Antidepressant Medication for Adults With Nonremitting Depression
Abstract
Objective: Adults with major depressive disorder frequently do not achieve remission with an initial treatment. Addition of psychotherapy for patients who do not achieve remission with antidepressant medication alone can target residual symptoms and protect against recurrence, but the utility of adding antidepressant medication after nonremission with cognitive-behavioral therapy (CBT) has received little study. The authors aimed to evaluate the acute and long-term outcomes resulting from both sequences of combination treatments.
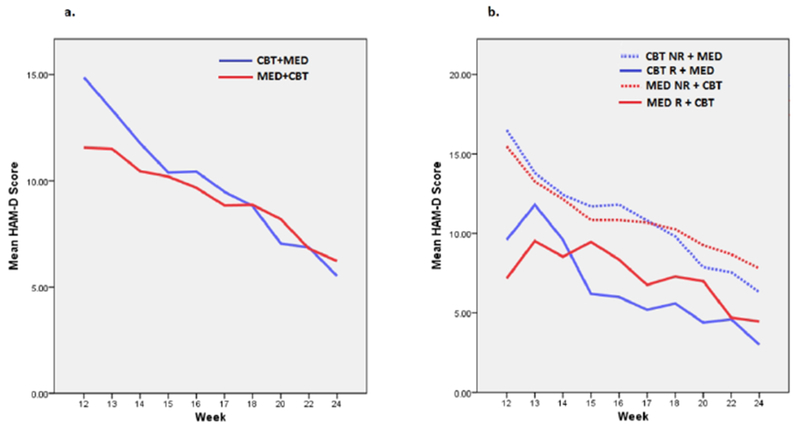
Methods: Previously untreated adults with major depression who were randomly assigned to receive escitalopram, duloxetine, or CBT monotherapy and completed 12 weeks of treatment without achieving remission entered an additional 12 weeks of combination treatment. For patients who did not achieve remission with CBT, escitalopram was added (CBT plus medication group) to their treatment, and for those who did not achieve remission with an antidepressant, CBT was added (medication plus CBT group) to their treatment. Patients who responded to the combination treatment entered an 18-month follow-up phase to assess risk of recurrence.
Results: A total of 112 patients who did not achieve remission with a monotherapy entered combination treatment (41 who responded to monotherapy but did not achieve remission and 71 who did not respond to monotherapy). Overall, remission rates after subsequent combination therapy were significantly higher among patients who responded to monotherapy but did not achieve remission (61%) than among patients who did not respond to monotherapy (41%). Among patients who responded to monotherapy but did not achieve remission, the remission rate in the CBT plus medication group (89%) was higher than in the medication plus CBT group (53%). However, among patients whose depression did not respond to monotherapy, rates of response and remission were similar between the treatment arms. Higher levels of anxiety, both prior to monotherapy and prior to beginning combination treatment, predicted poorer outcomes for both treatment groups.
Conclusions: The order in which CBT and antidepressant medication were sequentially combined did not appear to affect outcomes. Addition of an antidepressant is an effective approach to treating residual symptoms for patients who do not achieve remission with CBT, as is adding CBT after antidepressant monotherapy. Patients who do not respond to one treatment modality warrant consideration for addition of the alternative modality.
Keywords: Antidepressive Agent; Anxiety; Depression; Duloxetine; Escitalopram; Psychotherapy; Relapse.
Figures

Comment in
-
Treatment of Depression Versus Treatment of PTSD.Am J Psychiatry. 2019 Apr 1;176(4):259-261. doi: 10.1176/appi.ajp.2019.19020173. Am J Psychiatry. 2019. PMID: 30929505 No abstract available.
References
-
- Weitz E, Hollon SD, Twisk J, et al.: Does baseline depression severity moderate outcomes between CBT and pharmacotherapy? An individual participant data meta-analysis. JAMA Psychiatry 2015; 72:1102–1109 - PubMed
-
- Romera I, Perez V, Menchón JM, et al.: Social and occupational functioning impairment in patients in partial versus complete remission of a major depressive disorder episode. A six-month prospective epidemiological study. Eur Psychiatry 2010; 25:58–65 - PubMed
-
- Zimmerman M, Posternak MA, Chelminski I: Heterogeneity among depressed outpatients considered to be in remission. Compr Psychiatry 2007; 48:113–117 - PubMed
-
- Cuijpers P, De Wit L, Weitz E, et al.: The combination of psychotherapy and pharmacotherapy in the treatment of adult depression: a comprehensive meta-analysis. J Evid-Based Psychot 2015; 15:147–168
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
