

Maintenance of Gains, Morbidity, and Mortality at 1 Year Following Cardiac Rehabilitation in a Middle-Income Country: A Wait-List Control Crossover Trial
- PMID: 30764702
- PMCID: PMC6405675
- DOI: 10.1161/JAHA.118.011228
Maintenance of Gains, Morbidity, and Mortality at 1 Year Following Cardiac Rehabilitation in a Middle-Income Country: A Wait-List Control Crossover Trial
Abstract
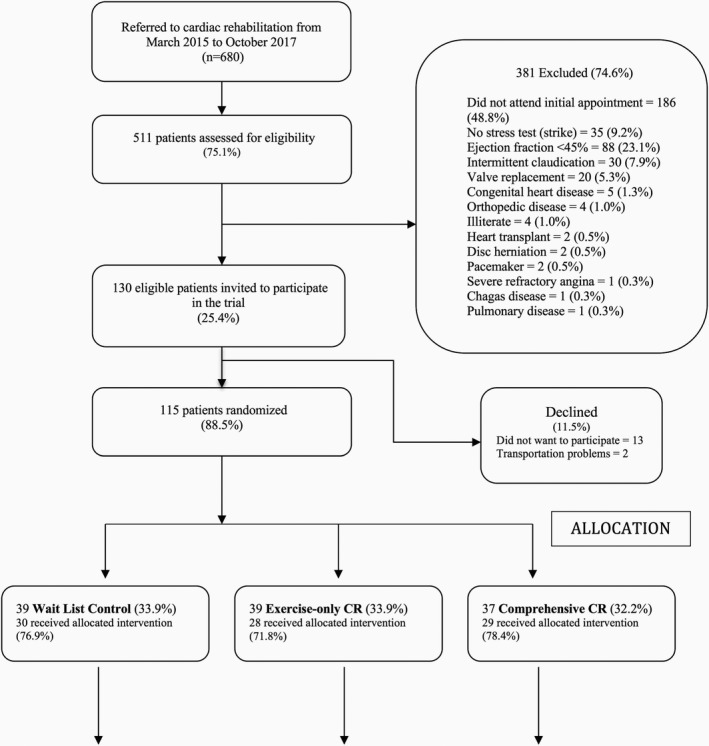
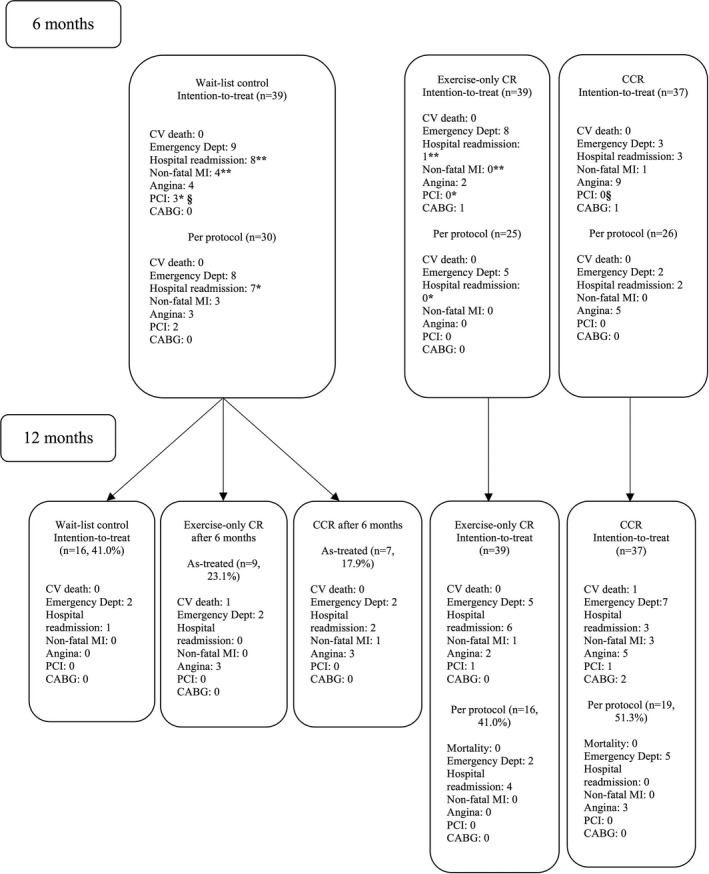
Background Despite the epidemic of cardiovascular diseases in middle-income countries, few trials are testing the benefits of cardiac rehabilitation ( CR ). This trial assessed (1) maintenance of functional capacity, risk factor control, knowledge, and heart-health behaviors and (2) mortality and morbidity at 6 months following CR in a middle-income country. Methods and Results Eligible Brazilian coronary patients were initially randomized (1:1:1 concealed) to 1 of 3 parallel arms (comprehensive CR [exercise plus education], exercise-only CR , or wait-list control). The CR programs were 6 months in duration, at which point follow-up assessments were performed. Mortality and morbidity were ascertained from chart and patient or family report (blinded). Controls were then offered CR (crossover). Outcomes were again assessed 6 months later (blinded). ANCOVA was performed for each outcome at 12 months. Overall, 115 (88.5%) patients were randomized, and 62 (53.9%) were retained at 1 year. At 6 months, 23 (58.9%) of those 39 initially randomized to the wait-list control elected to attend CR . Functional capacity, risk factors, knowledge, and heart-health behaviors were maintained from 6 to 12 months in participants from both CR arms (all P>0.05). At 1 year, knowledge was significantly greater with comprehensive CR at either time point ( P<0.001). There were 2 deaths. Hospitalizations ( P=0.03), nonfatal myocardial infarctions ( P=0.04), and percutaneous coronary interventions ( P=0.03) were significantly fewer with CR than control at 6 months. Conclusions CR participation is associated with lower morbidity, long-term maintenance of functional capacity, risk factors, and heart-health behaviors, as well as with greater cardiovascular knowledge compared with no CR . Clinical Trial Registration URL : http://www.clinicaltrials.gov . Unique identifier: NCT 02575976.
Trial registration: ClinicalTrials.gov NCT02575976.
Keywords: cardiac rehabilitation; coronary disease; morbidity/mortality; rehabilitation; risk factor.
Figures
References
-
- World Health Organization . Global Status Report on Noncommunicable Diseases. Geneva: WHO; 2014. Available at: http://www.who.int/nmh/publications/ncd-status-report-2014/en/. Accessed October 07, 2018.
-
- Brasil Ministério da Saúde . Sistema de Informações de Mortalidade SIM e IBGM. 2014. Available at: http://tabnet.datasus.gov.br/CGI/idb2006/matriz.htm. Accessed October 06, 2018.
-
- British Association for Cardiovascular Prevention and Rehabilitation . The BACPR Standards and Core Components for Cardiovascular Disease Prevention and Rehabilitation 2017. 3rd ed London: British Cardiovascular Society; 2017. Available at: http://www.bacpr.com/resources/BACPR_Standards_and_Core_Components_2017.pdf. Accessed December 14, 2018.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
