

Implementation science and stigma reduction interventions in low- and middle-income countries: a systematic review
- PMID: 30764820
- PMCID: PMC6376798
- DOI: 10.1186/s12916-018-1237-x
Implementation science and stigma reduction interventions in low- and middle-income countries: a systematic review
Abstract
Background: Interventions to alleviate stigma are demonstrating effectiveness across a range of conditions, though few move beyond the pilot phase, especially in low- and middle-income countries (LMICs). Implementation science offers tools to study complex interventions, understand barriers to implementation, and generate evidence of affordability, scalability, and sustainability. Such evidence could be used to convince policy-makers and donors to invest in implementation. However, the utility of implementation research depends on its rigor and replicability. Our objectives were to systematically review implementation studies of health-related stigma reduction interventions in LMICs and critically assess the reporting of implementation outcomes and intervention descriptions.
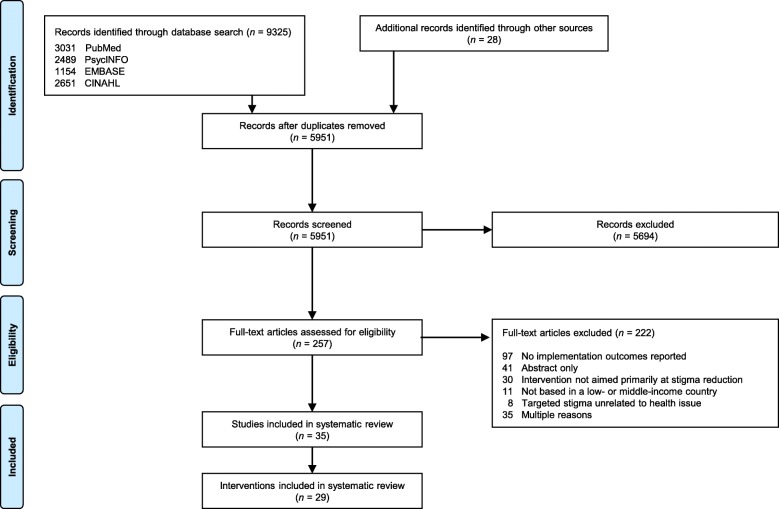
Methods: PubMed, CINAHL, PsycINFO, and EMBASE were searched for evaluations of stigma reduction interventions in LMICs reporting at least one implementation outcome. Study- and intervention-level characteristics were abstracted. The quality of reporting of implementation outcomes was assessed using a five-item rubric, and the comprehensiveness of intervention description and specification was assessed using the 12-item Template for Intervention Description and Replication (TIDieR).
Results: A total of 35 eligible studies published between 2003 and 2017 were identified; of these, 20 (57%) used qualitative methods, 32 (91%) were type 1 hybrid effectiveness-implementation studies, and 29 (83%) were evaluations of once-off or pilot implementations. No studies adopted a formal theoretical framework for implementation research. Acceptability (20, 57%) and feasibility (14, 40%) were the most frequently reported implementation outcomes. The quality of reporting of implementation outcomes was low. The 35 studies evaluated 29 different interventions, of which 18 (62%) were implemented across sub-Saharan Africa, 20 (69%) focused on stigma related to HIV/AIDS, and 28 (97%) used information or education to reduce stigma. Intervention specification and description was uneven.
Conclusion: Implementation science could support the dissemination of stigma reduction interventions in LMICs, though usage to date has been limited. Theoretical frameworks and validated measures have not been used, key implementation outcomes like cost and sustainability have rarely been assessed, and intervention processes have not been presented in detail. Adapted frameworks, new measures, and increased LMIC-based implementation research capacity could promote the rigor of future stigma implementation research, helping the field deliver on the promise of stigma reduction interventions worldwide.
Keywords: Stigma; implementation science; intervention; low- and middle-income countries; systematic review.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Link BG, Phelan JC. Conceptualizing stigma. Ann Rev Sociol. 2001;27:363–385. doi: 10.1146/annurev.soc.27.1.363. - DOI
-
- Thornicroft G, Mehta N, Clement S, Evans-Lacko S, Doherty M, Rose D, Koschorke M, Shidhaye R, O'Reilly C, Henderson C. Evidence for effective interventions to reduce mental-health-related stigma and discrimination. Lancet. 2016;387(10023):1123–32. - PubMed
-
- Sermrittirong S, Van Brakel WH, Bunbers-Aelen JF. How to reduce stigma in leprosy–a systematic. Lepr Rev. 2014;85:149–157. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
