

Serum KL-6 levels reflect the severity of interstitial lung disease associated with connective tissue disease
- PMID: 30764869
- PMCID: PMC6376648
- DOI: 10.1186/s13075-019-1835-9
Serum KL-6 levels reflect the severity of interstitial lung disease associated with connective tissue disease
Abstract
Background: Biomarkers have been actively investigated to supplement functional and imaging modalities to predict the severity, therapeutic responsiveness, and progression of connective tissue disease-associated interstitial lung disease (CTD-ILD). This study aimed to evaluate Krebs von den Lungen 6 (KL-6) as a potential biomarker reflecting the severity of CTD-ILD as assessed through computed tomography (CT) and pulmonary function test (PFT) parameters.
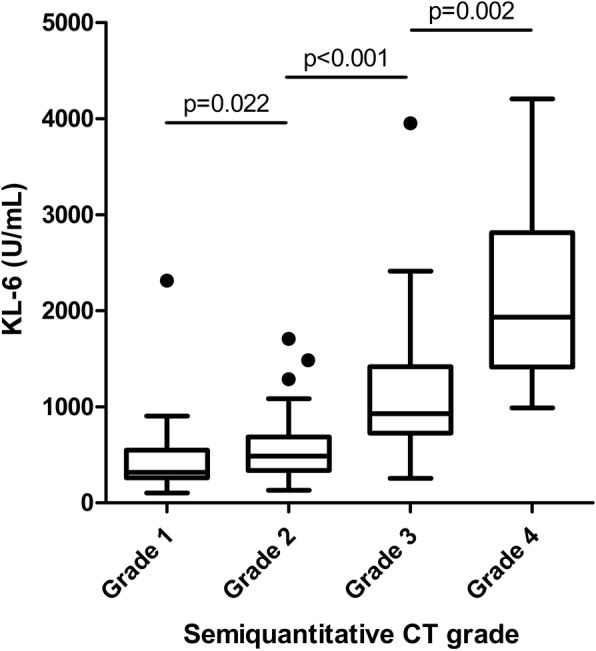
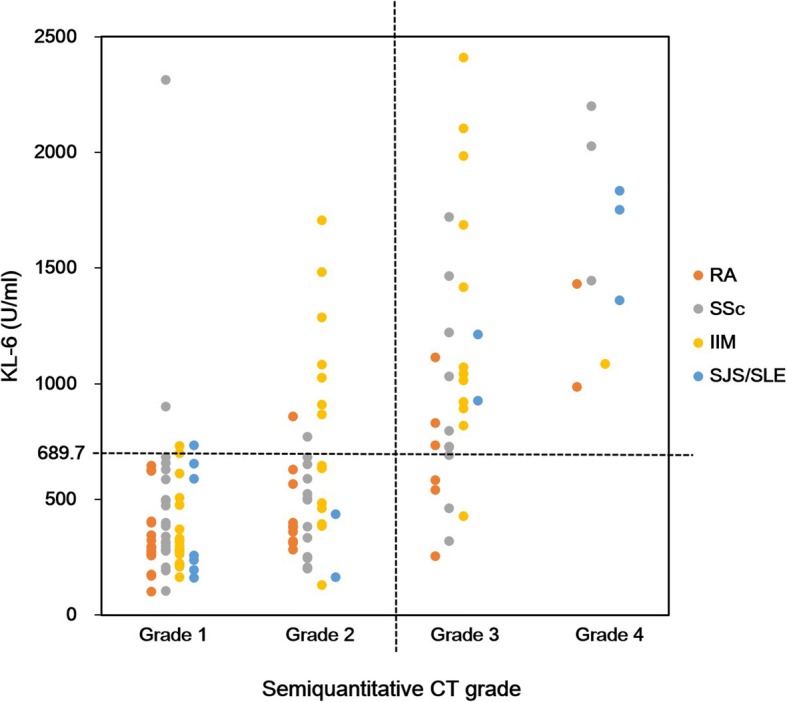
Methods: This retrospective study included 549 Korean patients with rheumatoid arthritis, systemic sclerosis, inflammatory myositis, and other CTDs with or without concurrent ILD. Serum KL-6 concentration (U/mL) was measured using the latex-enhanced immunoturbidimetric assay method. CT and PFT results were collected within 1 year of serum collection. A semiquantitative grade of ILD extent was evaluated through CT scan (grade 1, 0-25%; grade 2, 26-50%; grade 3, 51-75%; grade 4, 76-100%).
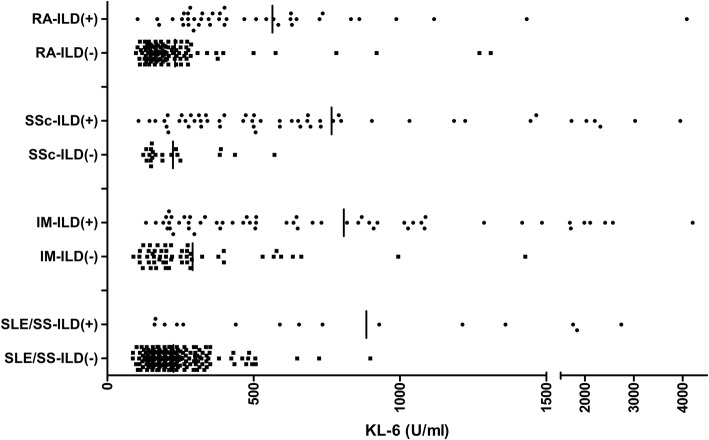
Results: CTD-ILD patients (n = 165) had elevated serum KL-6 levels compared to CTD patients without ILD (n = 384) (p < 0.001), and those findings were preserved after adjusting for age, sex, and CTD type. The semiquantitative grade of ILD on CT scan was significantly proportional to the KL-6 level, and the optimal cut-off KL-6 value effectively differentiated each ILD grade. The percent diffusing capacity of the lung for carbon monoxide (DLCO) (p < 0.001) and forced vital capacity (FVC) (p < 0.001) parameters had a moderate, negative correlation with the KL-6 level.
Conclusion: Serum KL-6 levels were increased in CTD-ILD patients and had a positive correlation with CT grade and a negative correlation with FVC and DLCO. Serum KL-6 levels may reflect CTD-ILD severity.
Keywords: Connective tissue disease; Interstitial lung disease; KL-6; Pulmonary function test.
Conflict of interest statement
Ethics approval and consent to participate
This study was performed in compliance with the Declaration of Helsinki and was approved by the Institutional Review Board of Seoul National University Hospital (IRB#:0408-131-010). All patients provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
