

Significance of anti-neutrophil cytoplasmic antibodies in systemic sclerosis
- PMID: 30764870
- PMCID: PMC6376778
- DOI: 10.1186/s13075-019-1839-5
Significance of anti-neutrophil cytoplasmic antibodies in systemic sclerosis
Abstract
Background: Up to 12% of patients with systemic sclerosis (SSc) have anti-neutrophil cytoplasmic antibodies (ANCA). However, the majority of these patients do not manifest ANCA-associated vasculitis (AAV) and the significance of ANCA in these patients is unclear. The aim of this study is to determine the prevalence of ANCA in a well-characterised SSc cohort and to examine the association between ANCA and SSc clinical characteristics, other autoantibodies, treatments and mortality.
Methods: Clinical data were obtained from 5 centres in the Australian Scleroderma Cohort Study (ASCS). ANCA positive was defined as the presence of any one or combination of cytoplasmic ANCA (c-ANCA), perinuclear ANCA (p-ANCA), atypical ANCA, anti-myeloperoxidase (anti-MPO) or anti-proteinase-3 (anti-PR3). Associations of demographic and clinical features with ANCA were investigated by logistic or linear regression. Survival analysis was performed using Kaplan-Meyer curves and Cox regression models.
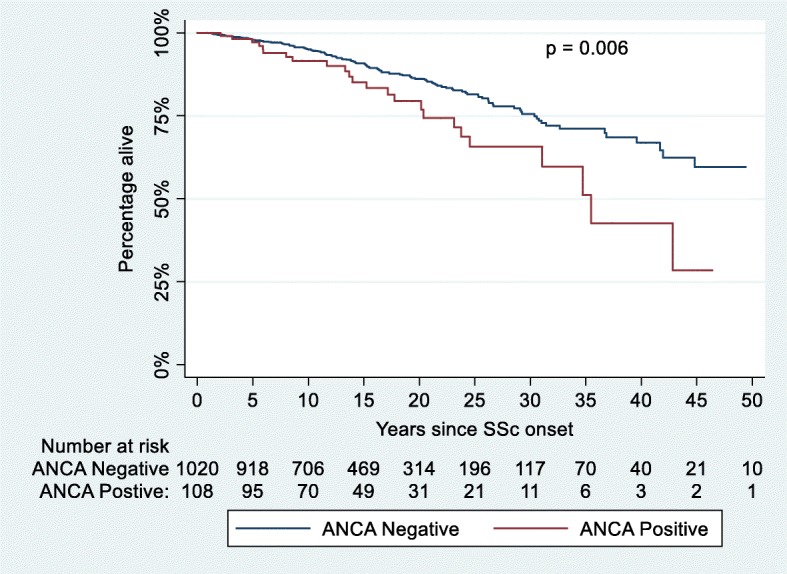
Results: Of 1303 patients, 116 (8.9%) were ANCA positive. Anti-PR3 was more common than anti-MPO (13.8% and 11.2% of ANCA-positive patients, respectively). Only 3 ANCA-positive patients had AAV. Anti-Scl-70 was more common in ANCA positive vs ANCA negative (25% vs 12.8%, p < 0.001), anti-MPO positive vs anti-MPO negative (38.5% vs 13.6%, p = 0.006) and anti-PR3 positive vs anti-PR3 negative patients (44.4% vs 13.4%, p < 0.001). A higher prevalence of interstitial lung disease (ILD) was found in the ANCA positive (44.8% vs 21.8%, p < 0.001) and the anti-PR3 positive groups (50.0% vs 23.4%, p = 0.009). In multivariable analysis, ANCA-positive status remained associated with ILD after adjusting for anti-Scl-70 antibodies. Pulmonary embolism (PE) was more common in ANCA-positive patients (8.6% vs 3.0%, p = 0.002) and anti-PR3-positive patients (16.7% vs 3.3%, p = 0.022). ANCA-positive status remained associated with PE in a multivariable analysis adjusting for anti-phospholipid antibodies. Kaplan-Meier analysis revealed increased mortality in ANCA-positive patients (p = 0.006). In Cox regression analysis, ANCA was associated with increased mortality, after adjusting for age and sex.
Conclusions: ANCA is associated with increased prevalence of ILD and PE in SSc. ANCA should be tested in SSc, as it identifies individuals with worse prognosis who require close monitoring for adverse outcomes.
Keywords: ANCA-associated vasculitis; Anti-neutrophil cytoplasmic antibodies (ANCA); Myeloperoxidase (MPO); Proteinase-3 (PR3); Systemic sclerosis (SSc).
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was provided by the Human Research Ethics Committee of the coordinating centre, St. Vincent's Hospital Melbourne (approval number HREC-A 020/07) and by each of the participating institutions (St Vincent’s Hospital, Melbourne and Monash Health, Victoria; John Hunter Hospital, New South Wales; Royal Adelaide Hospital, South Australia; Fiona Stanley Hospital, Western Australia).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
