

Numerical Simulations of Realistic Lead Trajectories and an Experimental Verification Support the Efficacy of Parallel Radiofrequency Transmission to Reduce Heating of Deep Brain Stimulation Implants during MRI
- PMID: 30765724
- PMCID: PMC6375985
- DOI: 10.1038/s41598-018-38099-w
Numerical Simulations of Realistic Lead Trajectories and an Experimental Verification Support the Efficacy of Parallel Radiofrequency Transmission to Reduce Heating of Deep Brain Stimulation Implants during MRI
Abstract
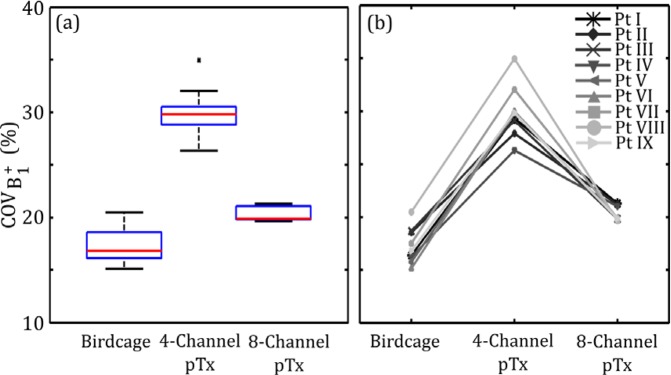
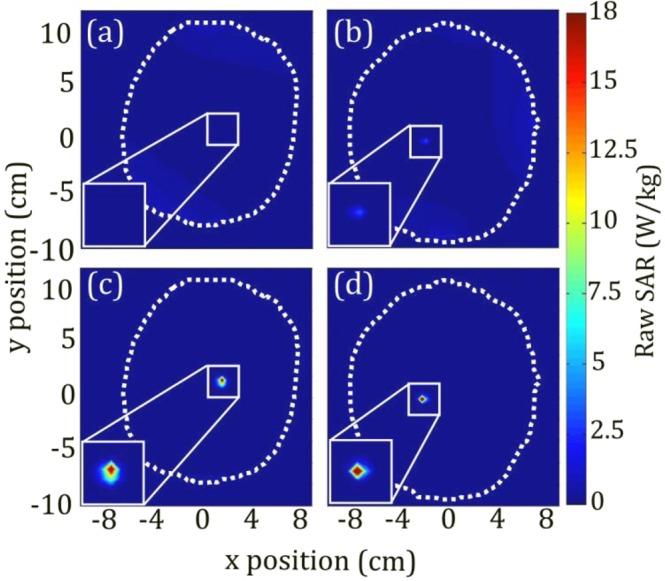
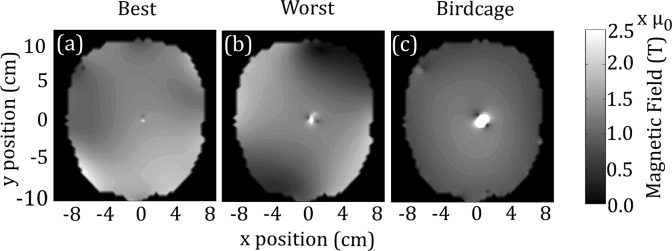
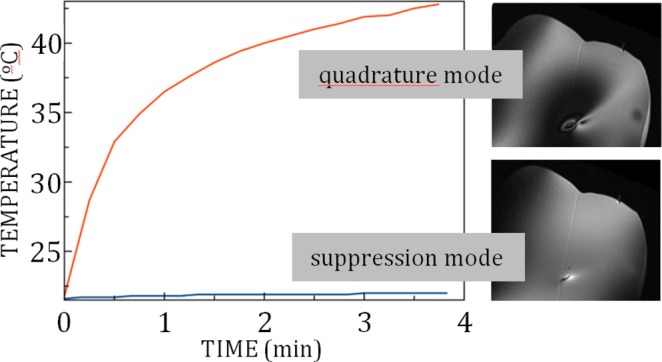
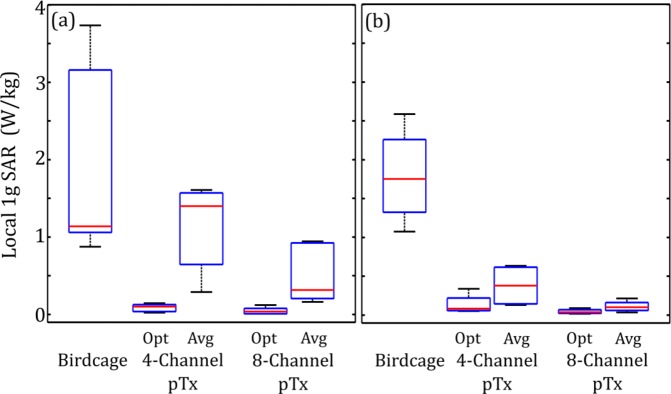
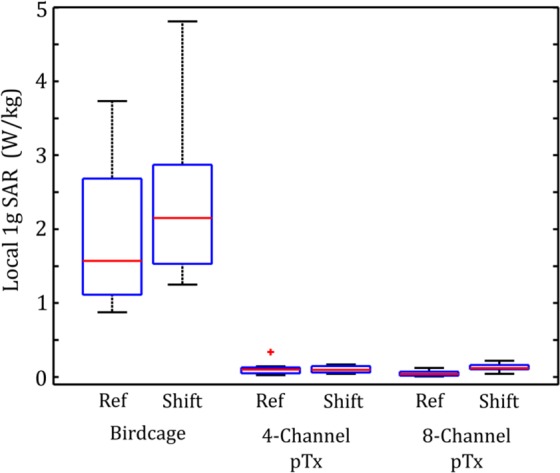
Patients with deep brain stimulation (DBS) implants may be subject to heating during MRI due to interaction with excitatory radiofrequency (RF) fields. Parallel RF transmit (pTx) has been proposed to minimize such RF-induced heating in preliminary proof-of-concept studies. The present work evaluates the efficacy of pTx technique on realistic lead trajectories obtained from nine DBS patients. Electromagnetic simulations were performed using 4- and 8-element pTx coils compared with a standard birdcage coil excitation using patient models and lead trajectories obtained by segmentation of computed tomography data. Numerical optimization was performed to minimize local specific absorption rate (SAR) surrounding the implant tip while maintaining spatial homogeneity of the transmitted RF magnetic field (B1+), by varying the input amplitude and phase for each coil element. Local SAR was significantly reduced at the lead tip with both 4-element and 8-element pTx (median decrease of 94% and 97%, respectively), whereas the median coefficient of spatial variation of B1+ inhomogeneity was moderately increased (30% for 4-element pTx and 20% for 8-element pTx) compared to that of the birdcage coil (17%). Furthermore, the efficacy of optimized 4-element pTx was verified experimentally by imaging a head phantom that included a wire implanted to approximate the worst-case lead trajectory for localized heating, based on the simulations. Negligible temperature elevation was observed at the lead tip, with reasonable image uniformity in the surrounding region. From this experiment and the simulations based on nine DBS patient models, optimized pTx provides a robust approach to minimizing local SAR with respect to lead trajectory.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
