

Quantitative nontumorous and tumorous human brain tissue assessment using microstructural co- and cross-polarized optical coherence tomography
- PMID: 30765763
- PMCID: PMC6375924
- DOI: 10.1038/s41598-019-38493-y
Quantitative nontumorous and tumorous human brain tissue assessment using microstructural co- and cross-polarized optical coherence tomography
Abstract
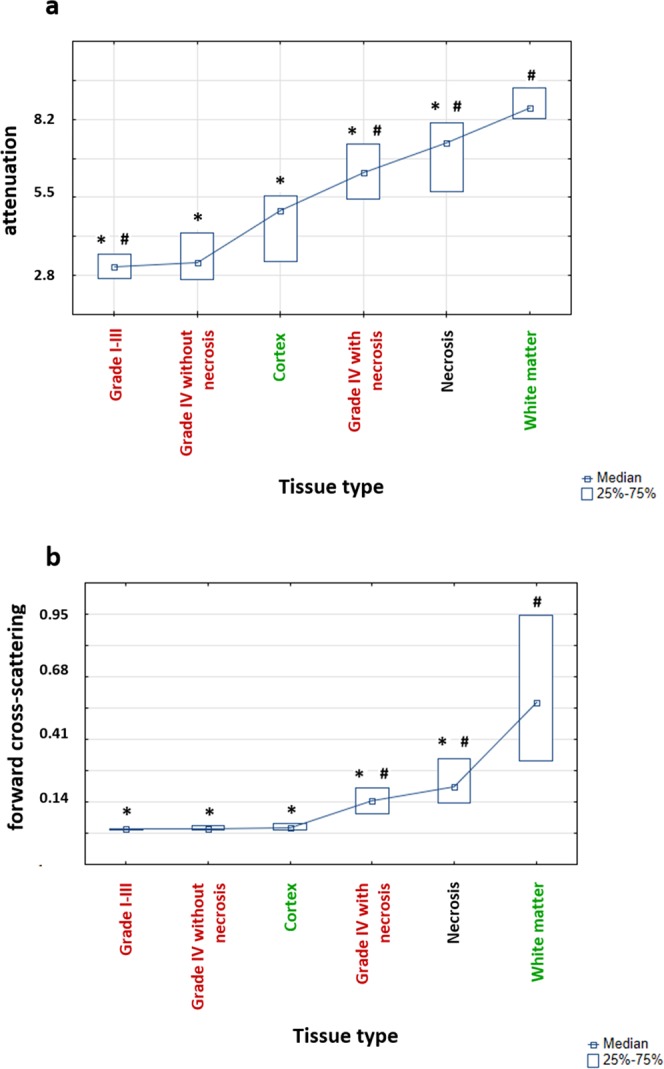
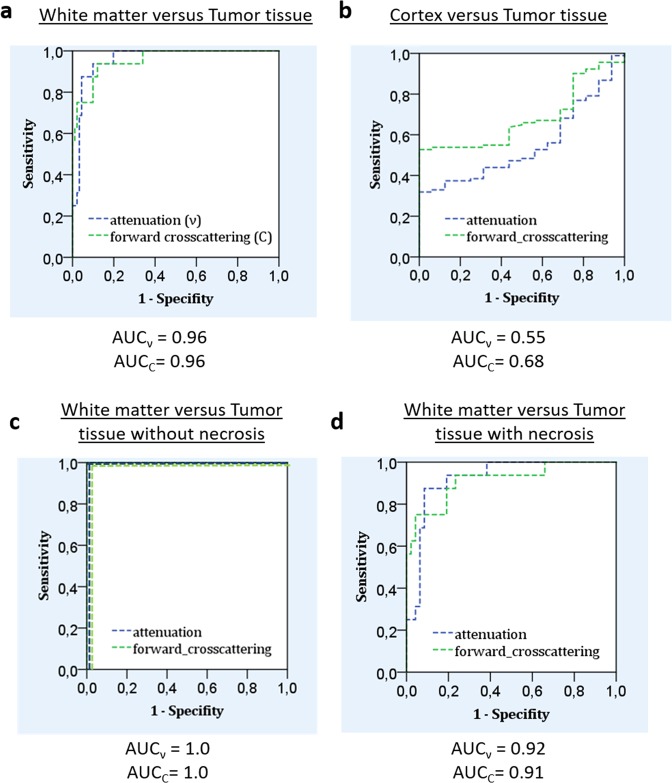
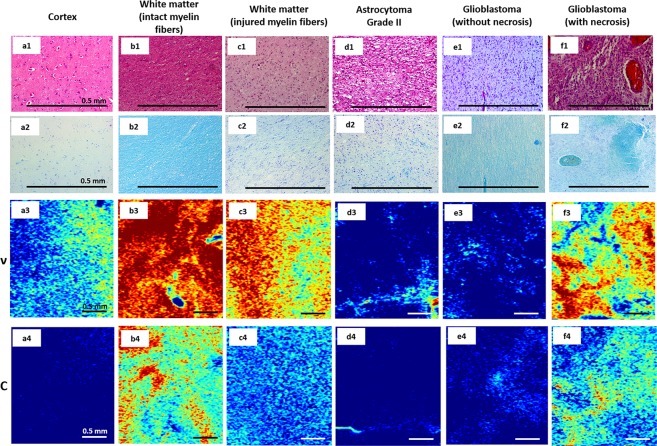
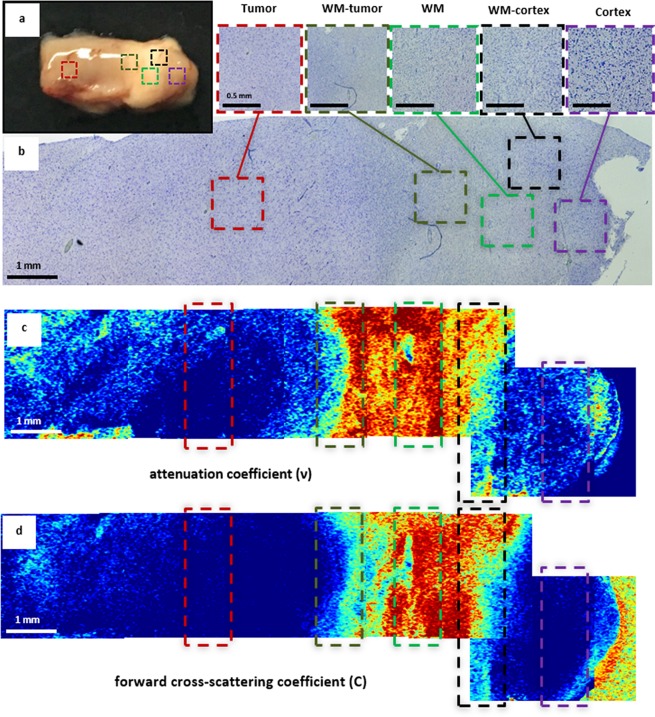
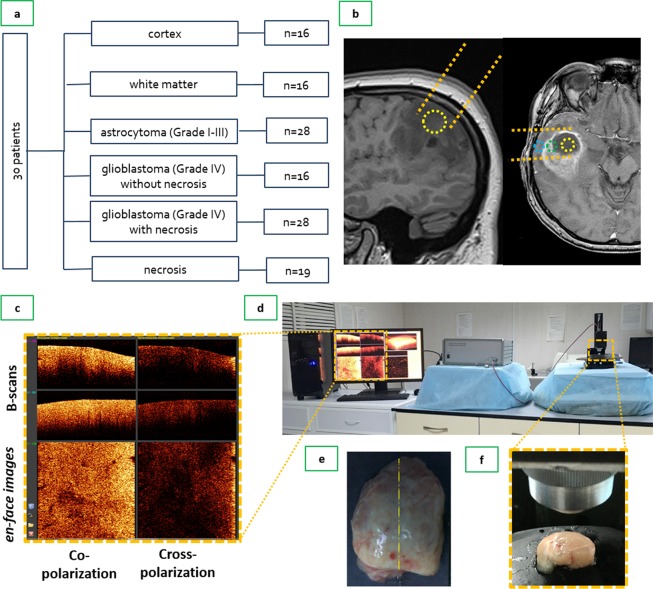
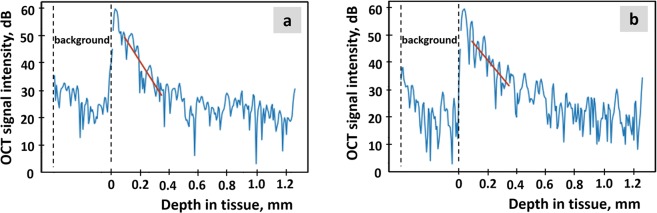
Optical coherence tomography (OCT) is a promising method for detecting cancer margins during tumor resection. This study focused on differentiating tumorous from nontumorous tissues in human brain tissues using cross-polarization OCT (CP OCT). The study was performed on fresh ex vivo human brain tissues from 30 patients with high- and low-grade gliomas. Different tissue types that neurosurgeons should clearly distinguish during surgery, such as the cortex, white matter, necrosis and tumorous tissue, were separately analyzed. Based on volumetric CP OCT data, tumorous and normal brain tissue were differentiated using two optical coefficients - attenuation and forward cross-scattering. Compared with white matter, tumorous tissue without necrotic areas had significantly lower optical attenuation and forward cross-scattering values. The presence of particular morphological patterns, such as necrosis and injured myelinated fibers, can lead to dramatic changes in coefficient values and create some difficulties in differentiating between tissues. Color-coded CP OCT maps based on optical coefficients provided a visual assessment of the tissue. This study demonstrated the high translational potential of CP OCT in differentiating tumorous tissue from white matter. The clinical use of CP OCT during surgery in patients with gliomas could increase the extent of tumor resection and improve overall and progression-free survival.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Almeida, J. P., Chaichana, K. L., Rincon-Torroella, J. & Quinones-Hinojosa, A. The Value of Extent of Resection of Glioblastomas: Clinical Evidence and Current Approach. Current Neurology and Neuroscience Reports15, 10.1007/s11910-014-0517-x (2014). - PubMed
-
- Sanai N, Berger MS. Glioma Extent of Resection and Its Impact on Patient Outcome. Neurosurgery. 2008;62:753–766. doi: 10.1227/01.neu.0000318159.21731.cf. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
