

Ex vivo organotypic culture system of precision-cut slices of human pancreatic ductal adenocarcinoma
- PMID: 30765891
- PMCID: PMC6376017
- DOI: 10.1038/s41598-019-38603-w
Ex vivo organotypic culture system of precision-cut slices of human pancreatic ductal adenocarcinoma
Abstract
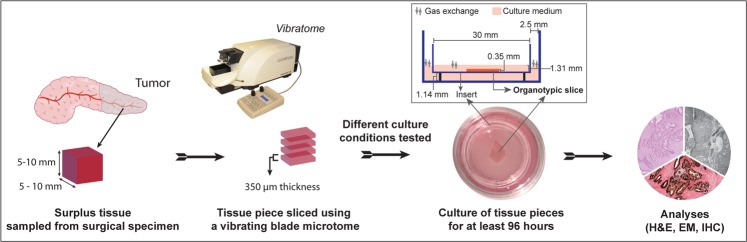
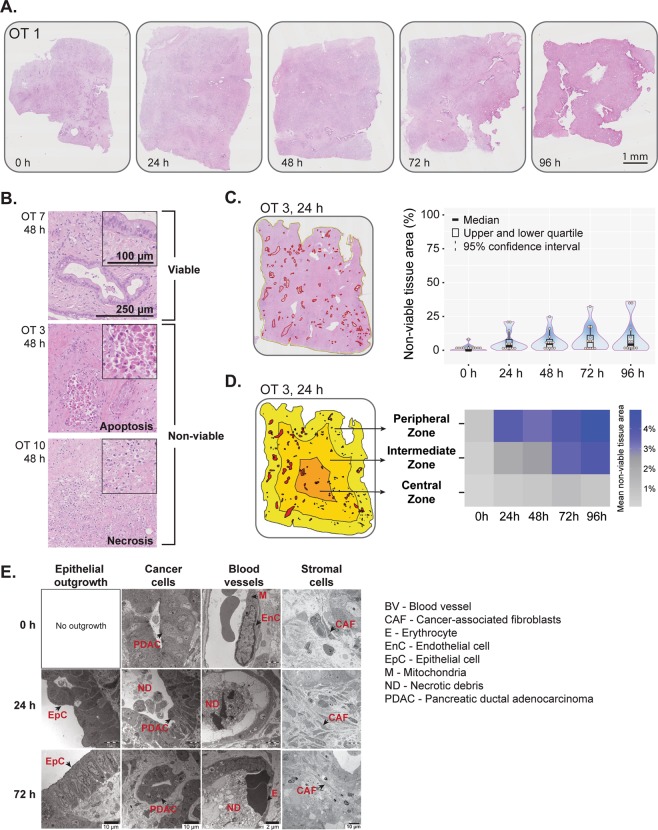
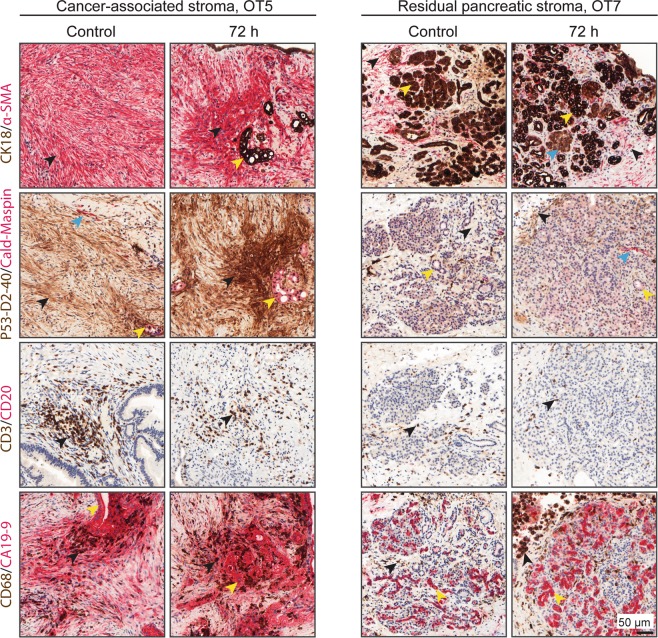
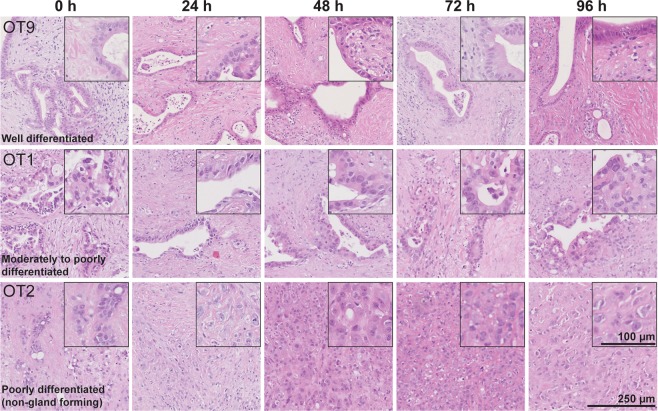
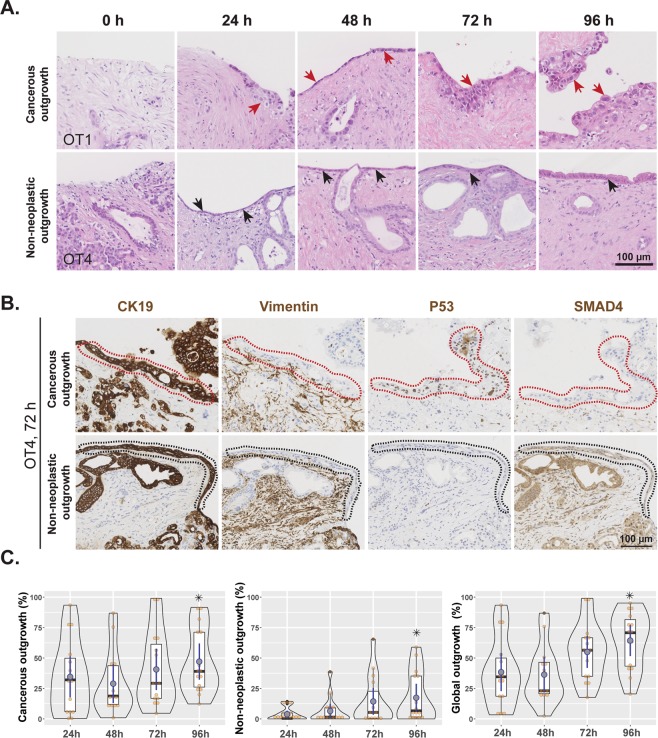
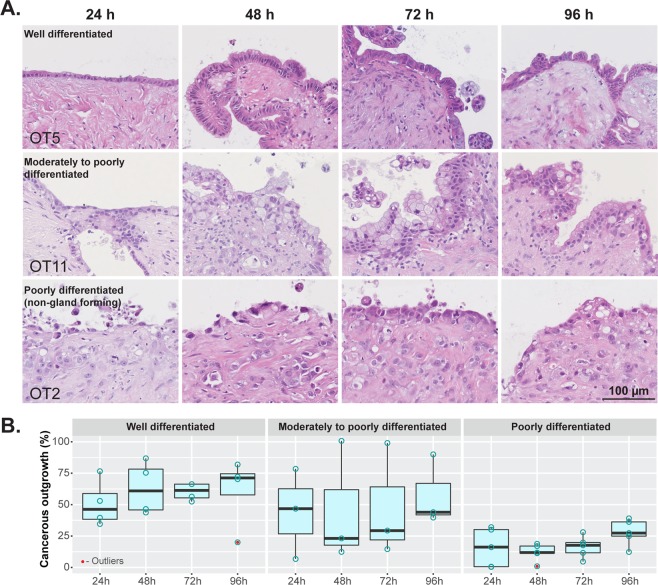
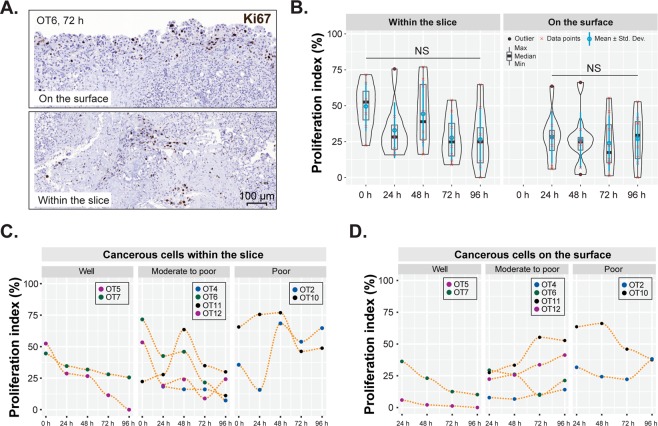
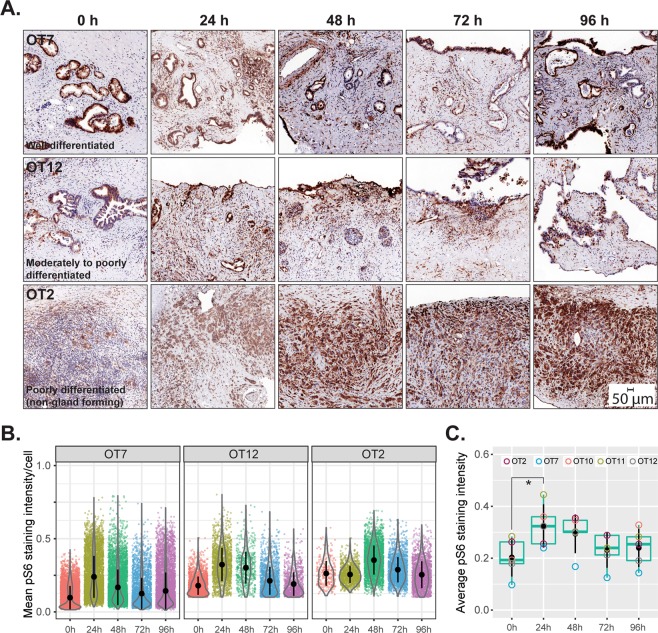
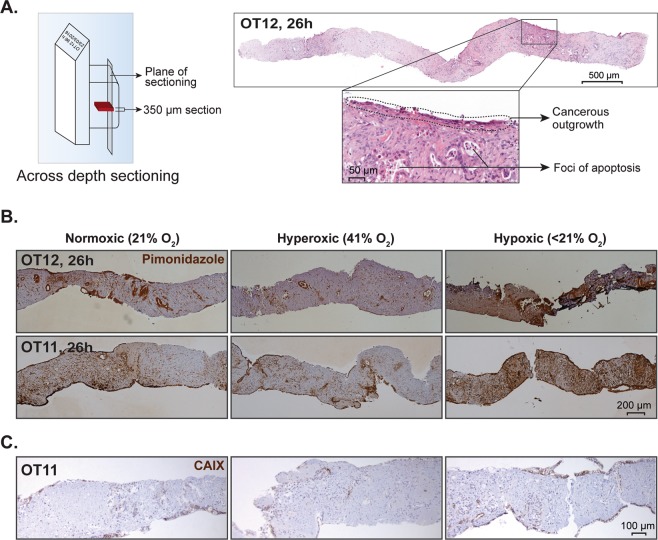
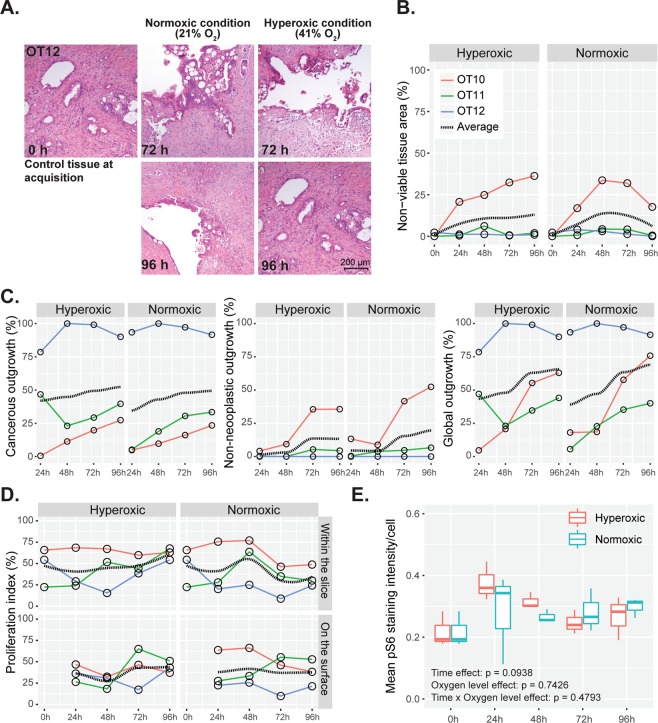
Pancreatic ductal adenocarcinoma (PDAC) has a poor prognosis, which is mainly due to late diagnosis and profound resistance to treatment. The latter is to a large extent attributed to the tumor stroma that is exceedingly prominent in PDAC and engages in complex interactions with the cancer cells. Hence, relevant preclinical models of PDAC should also include the tumor stroma. We herein describe the establishment and functional validation of an ex vivo organotypic culture of human PDAC that is based on precision-cut tissue slices from surgical specimens and reproducibly recapitulates the complex cellular and acellular composition of PDAC, including its microenvironment. The cancer cells, tumor microenvironment and interspersed remnants of nonneoplastic pancreas contained in these 350 µm thick slices maintained their structural integrity, phenotypic characteristics and functional activity when in culture for at least 4 days. In particular, tumor cell proliferation persisted and the grade of differentiation and morphological phenotype remained unaltered. Cultured tissue slices were metabolically active and responsive to rapamycin, an mTOR inhibitor. This culture system is to date the closest surrogate to the parent carcinoma and harbors great potential as a drug sensitivity testing system for the personalized treatment of PDAC.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Löhr, J.-M. Pancreatic cancer should be treated as a medical emergency. BMJ: British Medical Journal349 (2014). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
