

Diagnostic Yield and Complication of Frameless Stereotactic Brain Biopsy
- PMID: 30765975
- PMCID: PMC6337997
- DOI: 10.4103/jnrp.jnrp_166_18
Diagnostic Yield and Complication of Frameless Stereotactic Brain Biopsy
Abstract
Background: With the advancement of neuronavigation technologies, frameless stereotactic brain biopsy has been developed. Previous studies proved that frameless stereotactic brain biopsy was as effective and safe as frame-based stereotactic brain biopsy. The authors aimed to find the factors associated with diagnostic yield and complication rate of frameless intracranial biopsy.
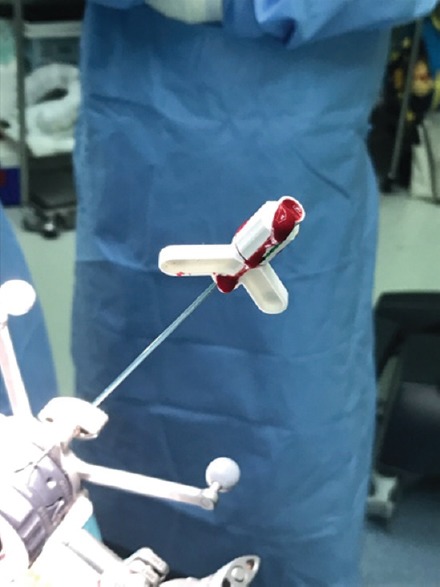
Materials and methods: Frameless stereotactic brain biopsy procedures, between March 2009 and April 2017, were retrospectively reviewed from medical records including imaging studies. Using logistic regression analysis, various factors were analyzed for association with diagnostic yield and postoperative complications.
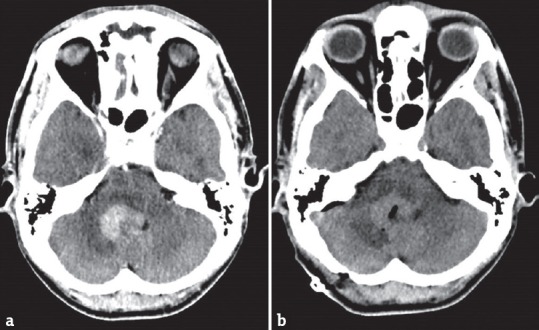
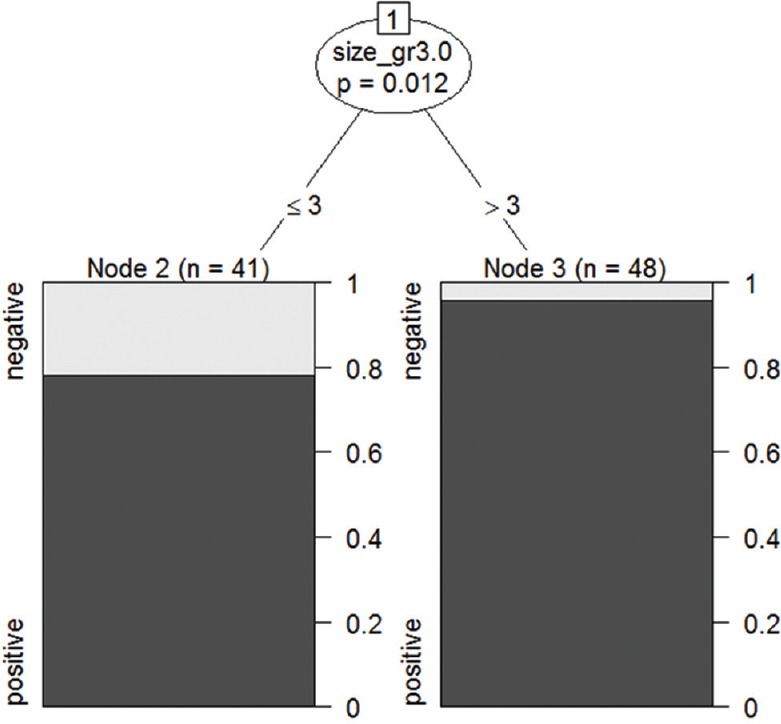
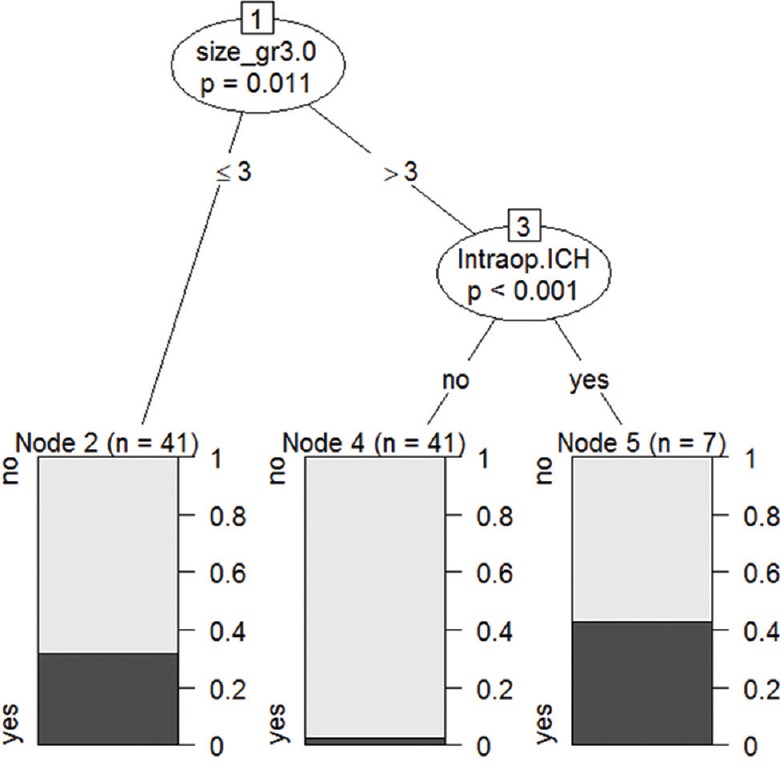
Results: Eighty-nine frameless stereotactic brain biopsy procedures were performed on 85 patients. The most common pathology was primary central nervous system lymphoma (43.8%), followed by low-grade glioma (15.7%), and high-grade glioma (15%), respectively. The diagnostic yield was 87.6%. Postoperative intracerebral hematoma occurred in 19% of cases; however, it was symptomatic in only one case. The size of the lesion was associated with both diagnostic yield and postoperative intracerebral hematoma complication. Lesions, larger than 3 cm in diameter, were associated with a higher rate of positive biopsy result (P = 0.01). Lesion 3 cm or smaller than 3 cm in diameter, and intraoperative bleeding associated with a higher percentage of postoperative intracerebral hematoma complications (P = 0.01).
Conclusions: For frameless stereotactic brain biopsy, the size of the lesion is the essential factor determining diagnostic yield and postoperative intracerebral hematoma complication.
Keywords: Diagnostic yield; frameless stereotactic brain biopsy; neuronavigation.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Woodworth GF, McGirt MJ, Samdani A, Garonzik I, Olivi A, Weingart JD, et al. Frameless image-guided stereotactic brain biopsy procedure: Diagnostic yield, surgical morbidity, and comparison with the frame-based technique. J Neurosurg. 2006;104:233–7. - PubMed
-
- Smith JS, Quiñones-Hinojosa A, Barbaro NM, McDermott MW. Frame-based stereotactic biopsy remains an important diagnostic tool with distinct advantages over frameless stereotactic biopsy. J Neurooncol. 2005;73:173–9. - PubMed
-
- Dammers R, Haitsma IK, Schouten JW, Kros JM, Avezaat CJ, Vincent AJ. Safety and efficacy of frameless and frame-based intracranial biopsy techniques. Acta Neurochir (Wien) 2008;150:23–9. - PubMed
-
- Nishihara M, Takeda N, Harada T, Kidoguchi K, Tatsumi S, Tanaka K, et al. Diagnostic yield and morbidity by neuronavigation-guided frameless stereotactic biopsy using magnetic resonance imaging and by frame-based computed tomography-guided stereotactic biopsy. Surg Neurol Int. 2014;5:S421–6. - PMC - PubMed
-
- Frati A, Pichierri A, Bastianello S, Raco A, Santoro A, Esposito V, et al. Frameless stereotactic cerebral biopsy: Our experience in 296 cases. Stereotact Funct Neurosurg. 2011;89:234–45. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous