

The Efficacy of Vortioxetine on Anhedonia in Patients With Major Depressive Disorder
- PMID: 30766492
- PMCID: PMC6365446
- DOI: 10.3389/fpsyt.2019.00017
The Efficacy of Vortioxetine on Anhedonia in Patients With Major Depressive Disorder
Abstract
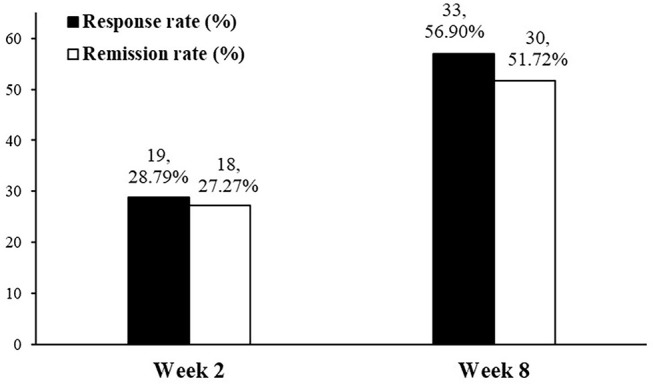
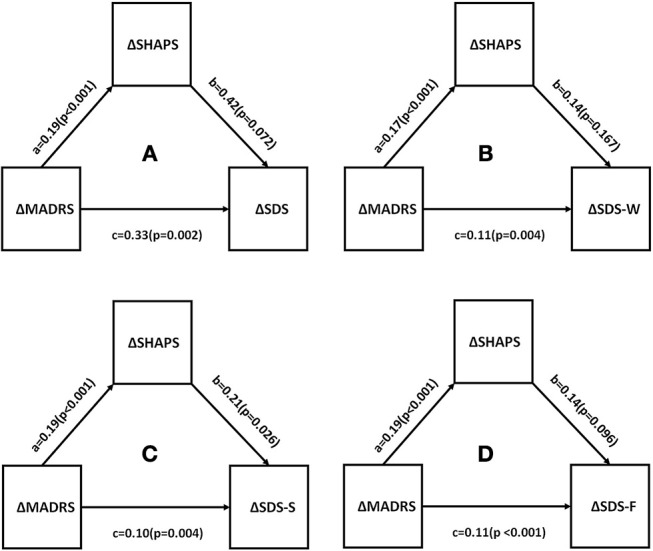
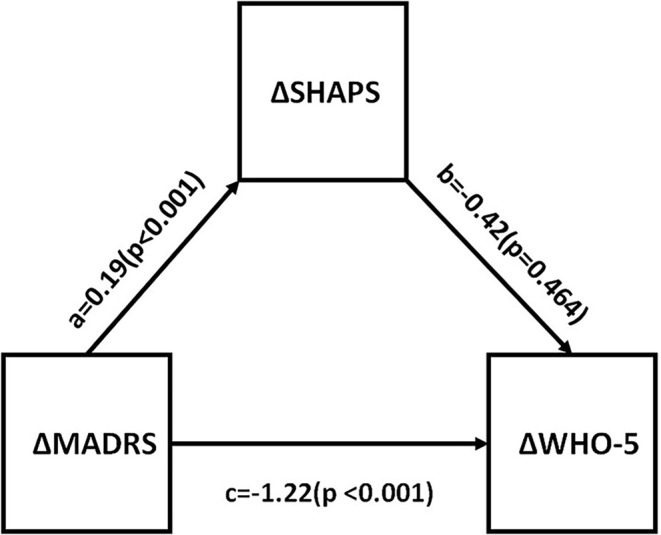
Background: Anhedonia is a common, persistent, and disabling phenomenon in treated adults with Major Depressive Disorder (MDD). Hitherto, relatively few antidepressant agents have been evaluated with respect to their effect on anhedonia in MDD. Methods: This is a post-hoc analysis of a primary study that sought to evaluate the sensitivity to change of the THINC-integrated tool (THINC-it) in MDD (ClinicalTrials.gov Identifier: NCT03053362). Adults meeting DSM-5 criteria for MDD with at least moderate depressive symptom severity [i.e., Montgomery Åsberg Depression Rating Scale (MADRS) total score ≥20] were eligible. Subjects were recruited between October 2017 and August 2018 in Toronto, Ontario at the Brain and Cognition Discovery Foundation. All subjects received open-label vortioxetine (10-20 mg/day, flexibly-dosed) for 8 weeks. Herein, the primary outcome of interest was the change from baseline to endpoint in the Snaith-Hamilton Pleasure Scale (SHAPS) total score, as well as the MADRS anhedonia factor. The mediational effects of improvements in anhedonia on general function and quality of life, as measured by the Sheehan Disability Scale (SDS) and the 5-Item World Health Organization Well-Being Index (WHO-5), were secondarily assessed. Results: A total of 100 subjects with MDD were enrolled in the primary study and began treatment with vortioxetine. Vortioxetine significantly improved anhedonia as evidenced by significant baseline to endpoint improvements in SHAPS and MADRS anhedonia factor scores (p < 0.0001). Improvements in the SHAPS and the MADRS anhedonia factor correlated with improvements in general function (i.e., SDS) and quality of life (i.e., WHO-5) (p < 0.0001). Notably, improvements in anhedonia were found to mediate the association between improvements in overall depressive symptom severity (i.e., MADRS total score) and social functioning (i.e., social life component of the SDS) (p = 0.026). Conclusion: The unmet need in depression is to improve patient functioning and other patient-reported outcomes (e.g., quality of life). Antidepressant interventions capable of attenuating anhedonia as well as cognitive dysfunction in MDD may help in this regard, as improvement in these domains have been associated with improvement in psychosocial function and quality of life.
Keywords: anhedonia; antidepressants; function; major depressive disorder; quality of life; vortioxetine.
Figures
References
-
- Vos T, Abajobir A, Abbafati C, Abbas K, Abate K, Abd-Allah F. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet (2017) 390:1211–59. 10.1016/S0140-6736(17)32154-2 - DOI - PMC - PubMed
-
- APA Diagnostic and Statistical Manual of Mental Disorder. 5th ed. American Psychiatric Association; (2013). 10.1176/appi.books.9780890425596 - DOI
-
- NIMH Definitions of the RDoC Domains and Constructs (2018). Available online at: https://www.nimh.nih.gov/research-priorities/rdoc/definitions-of-the-rdo...
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical