

Can Intestinal Pseudo-Obstruction Drive Recurrent Stroke-Like Episodes in Late-Onset MELAS Syndrome? A Case Report and Review of the Literature
- PMID: 30766507
- PMCID: PMC6365425
- DOI: 10.3389/fneur.2019.00038
Can Intestinal Pseudo-Obstruction Drive Recurrent Stroke-Like Episodes in Late-Onset MELAS Syndrome? A Case Report and Review of the Literature
Abstract
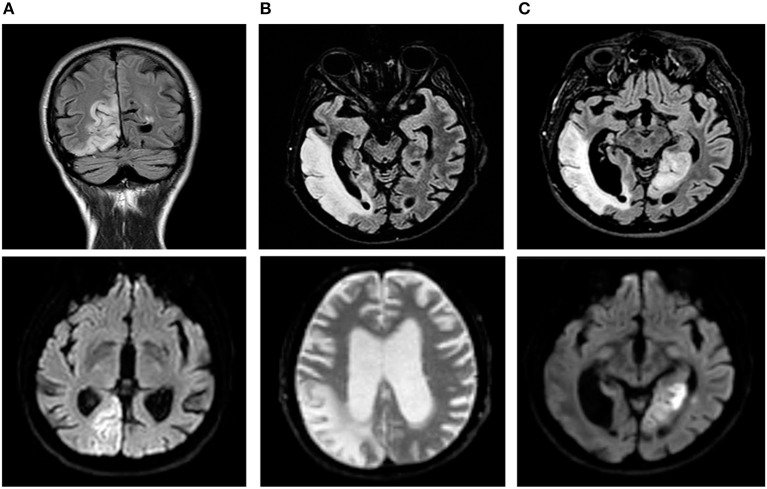
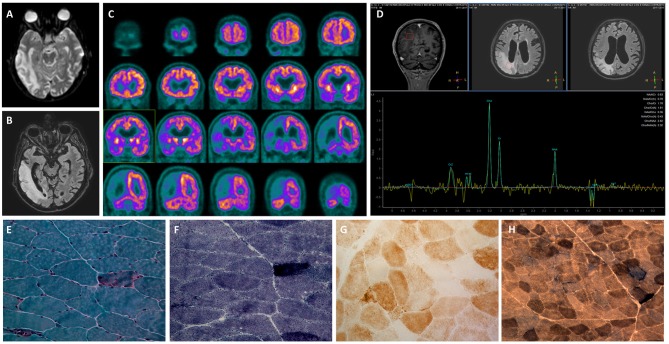
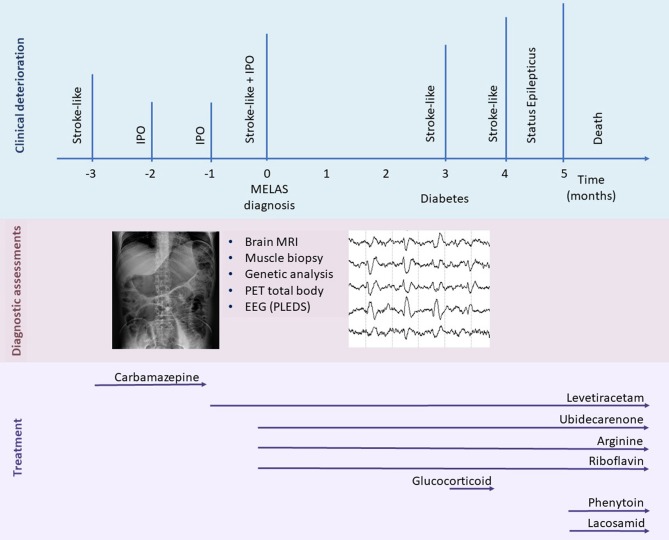
Mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS) syndrome is a maternally inherited mitochondrial disorder that is most commonly caused by the m. 3243A>G mutation in the MT-TL1 mitochondrial DNA gene, resulting in impairment of mitochondrial energy metabolism. Although childhood is the typical age of onset, a small fraction (1-6%) of individuals manifest the disease after 40 years of age and usually have a less aggressive disease course. The clinical manifestations are variable and mainly depend on the degree of heteroplasmy in the patient's tissues and organs. They include muscle weakness, diabetes, lactic acidemia, gastrointestinal disturbances, and stroke-like episodes, which are the most commonly observed symptom. We describe the case of a 50-year-old male patient who presented with relapsing intestinal pseudo-obstruction (IPO) episodes, which led to a late diagnosis of MELAS. After diagnosis, he presented several stroke-like episodes in a short time period and developed a rapidly progressive cognitive decline, which unfortunately resulted in his death. We describe the variable clinical manifestations of MELAS syndrome in this atypical and relatively old patient, with a focus on paralytic ileus and stroke-like episodes; the first symptom may have driven the others, leading to a relentless decline. Moreover, we provide a brief revision of previous reports of IPO occurrence in MELAS patients with the m.3243A>G mutation, and we investigate its relationship with stroke-like episodes. Our findings underscore the importance of recognizing gastrointestinal disturbance to prevent neurological comorbidities.
Keywords: MELAS; gastrointestinal disturbance; intestinal pseudo-obstruction; mitochondrial disorders; stroke-like episodes.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases