

Proenkephalin and prognosis in heart failure with preserved ejection fraction: a GREAT network study
- PMID: 30767059
- PMCID: PMC6652170
- DOI: 10.1007/s00392-019-01424-y
Proenkephalin and prognosis in heart failure with preserved ejection fraction: a GREAT network study
Abstract
Background: Proenkephalin (PENK), a stable endogenous opioid biomarker related to renal function, has prognostic utility in acute and chronic heart failure. We investigated the prognostic utility of PENK in heart failure with preserved ejection fraction (HFpEF), and its relationship to renal function, Body Mass Index (BMI), and imaging measures of diastolic dysfunction.
Methods: In this multicentre study, PENK was measured in 522 HFpEF patients (ejection fraction > 50%, 253 male, mean age 76.13 ± 10.73 years) and compared to 47 age and sex-matched controls. The primary endpoint was 2-years composite of all-cause mortality and/or heart failure rehospitalisation (HF). A subset (n = 163) received detailed imaging studies.
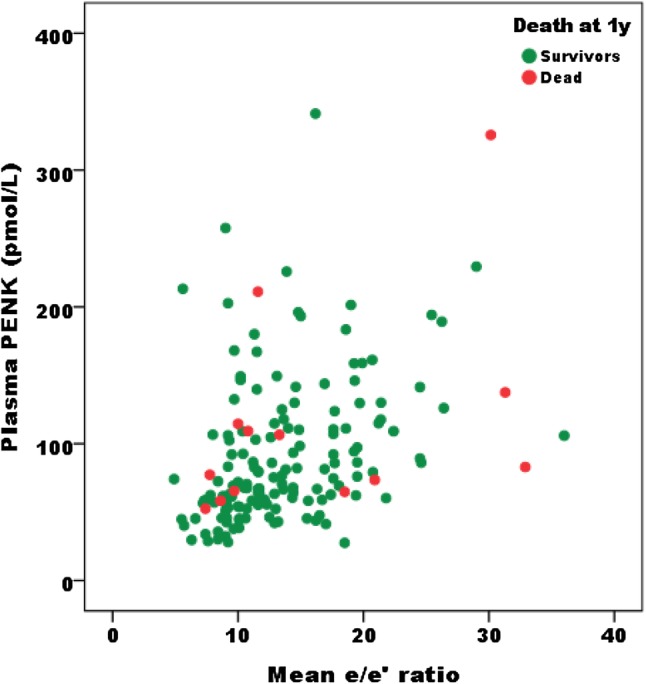
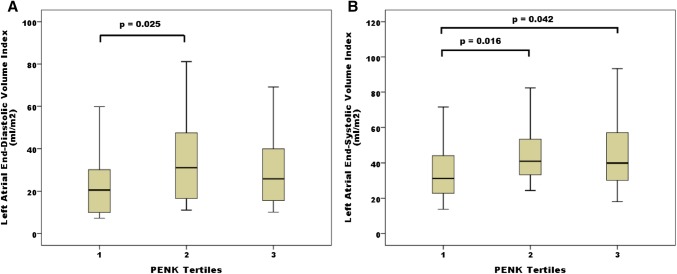
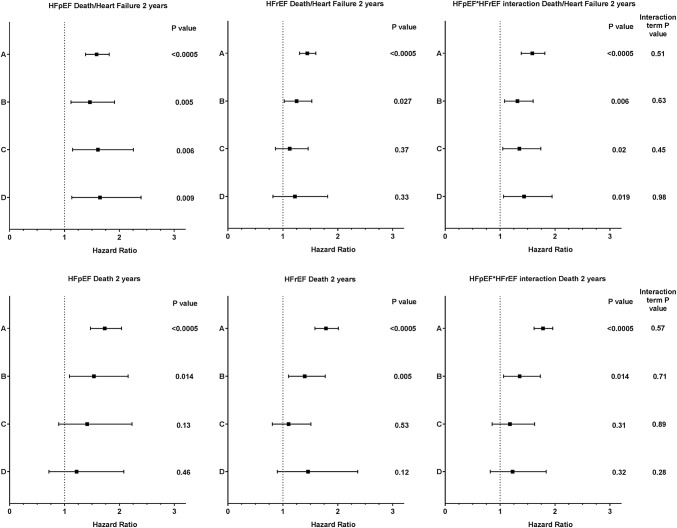
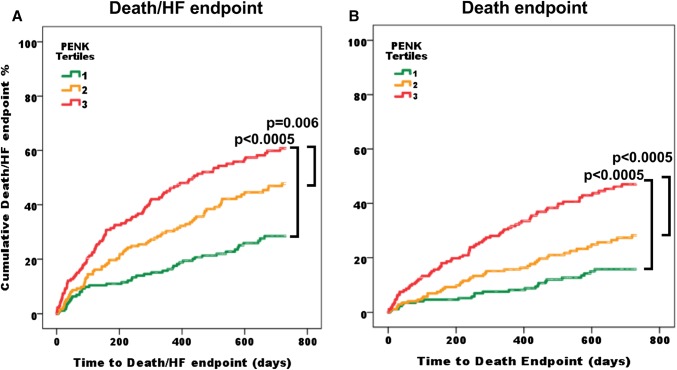
Results: PENK levels were raised in HFpEF (median [interquartile range] 88.9 [62.1-132.0]) compared to normal controls (56.3 [47.9-70.5]). PENK was correlated to urea, eGFR, Body Mass Index and E/e' (rs 0.635, - 0.741, - 0.275, 0.476, respectively, p < 0.0005). During 2 years follow-up 144 patients died and 220 had death/HF endpoints. Multivariable Cox regression models showed PENK independently predicted 2 year death/HF [hazard ratio (for 1 SD increment of log-transformed biomarker) HR 1.45 [95% CI 1.12-1.88, p = 0.005]], even after adjustment for troponin (HR 1.59 [1.14-2.20, p = 0.006]), and Body Mass Index (HR 1.63 [1.13-2.33, p = 0.009]). PENK showed no interaction with ejection fraction status for prediction of poor outcomes. Net reclassification analyses showed PENK significantly improved classification of death/HF outcomes for multivariable models containing natriuretic peptide, troponin and Body Mass Index (p < 0.05 for all).
Conclusions: In HFpEF, PENK levels are related to BMI, and measures of diastolic dysfunction and are prognostic for all-cause mortality and heart failure rehospitalisation.
Keywords: B-type natriuretic peptide; Heart failure; Opioids; Preserved ejection fraction; Proenkephalin; Renal function.
Conflict of interest statement
Dr. Bergmann holds ownership in Sphingotec GmbH which manufactures the PENK assay, and is a member of the board of directors of Sphingotec GmbH. Dr. Struck is an employee of Sphingotec GmbH which manufactures the PENK assay. Dr. Mueller has received research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union, the Cardiovascular Research Foundation Basel, the University Hospital Basel, Abbott, Astra Zeneca, Beckman Coulter, BG medicine, Biomerieux, BRAHMS, Critical Diagnostics, Nanosphere, Roche, Siemens, Singulex, Sphingotec, 8sense as well as speaker/consulting honoraria from Abbott, Alere, Astra Zeneca, Biomerieux, BMS, Boehringer Ingelheim, BRAHMS, Cardiorentis, Eli Lilly, Novartis, Roche, Sanofi, Siemens, and Singulex. Dr Squire has received research grants from Novartis AG and Servier as well as speaker/consulting honoraria from Novartis. The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Proenkephalin, Renal Dysfunction, and Prognosis in Patients With Acute Heart Failure: A GREAT Network Study.J Am Coll Cardiol. 2017 Jan 3;69(1):56-69. doi: 10.1016/j.jacc.2016.10.038. J Am Coll Cardiol. 2017. PMID: 28057251
-
Proenkephalin and prognosis after acute myocardial infarction.J Am Coll Cardiol. 2014 Jan 28;63(3):280-9. doi: 10.1016/j.jacc.2013.09.037. Epub 2013 Oct 16. J Am Coll Cardiol. 2014. PMID: 24140658
-
Proenkephalin, an Opioid System Surrogate, as a Novel Comprehensive Renal Marker in Heart Failure.Circ Heart Fail. 2019 May;12(5):e005544. doi: 10.1161/CIRCHEARTFAILURE.118.005544. Circ Heart Fail. 2019. PMID: 31091993
-
Comprehensive Assessment of Heart Failure with Preserved Ejection Fraction Using Cardiac MRI.Heart Fail Clin. 2021 Jul;17(3):447-462. doi: 10.1016/j.hfc.2021.03.006. Heart Fail Clin. 2021. PMID: 34051976 Review.
-
Renal Dysfunction and Heart Failure with Preserved Ejection Fraction.Heart Fail Clin. 2021 Jul;17(3):357-367. doi: 10.1016/j.hfc.2021.03.005. Heart Fail Clin. 2021. PMID: 34051968 Review.
Cited by
-
Integrated microarray analysis to identify potential biomarkers and therapeutic targets in dilated cardiomyopathy.Mol Med Rep. 2020 Aug;22(2):915-925. doi: 10.3892/mmr.2020.11145. Epub 2020 May 14. Mol Med Rep. 2020. PMID: 32626989 Free PMC article.
-
Proenkephalin and the risk of new-onset heart failure: data from prevention of renal and vascular end-stage disease.Clin Cardiol. 2021 Dec;44(12):1662-1672. doi: 10.1002/clc.23729. Epub 2021 Oct 30. Clin Cardiol. 2021. PMID: 34716603 Free PMC article.
-
Proenkephalin (PENK): a functional biomarker in chronic kidney diseases - hope or just a new bystander?J Nephrol. 2025 Apr 15. doi: 10.1007/s40620-025-02268-8. Online ahead of print. J Nephrol. 2025. PMID: 40234363 Review.
-
Proenkephalin: A New Biomarker for Glomerular Filtration Rate and Acute Kidney Injury.Nephron. 2020;144(12):655-661. doi: 10.1159/000509352. Epub 2020 Jul 31. Nephron. 2020. PMID: 32739920 Free PMC article. Review.
-
Association between Proenkephalin A and cardiovascular outcomes in ambulatory Veterans.Int J Cardiol Heart Vasc. 2024 Nov 16;55:101557. doi: 10.1016/j.ijcha.2024.101557. eCollection 2024 Dec. Int J Cardiol Heart Vasc. 2024. PMID: 39633843 Free PMC article.
References
-
- Anand IS, Rector TS, Cleland JG, et al. Prognostic value of baseline plasma amino-terminal pro-brain natriuretic peptide and its interactions with irbesartan treatment effects in patients with heart failure and preserved ejection fraction: findings from the I-PRESERVE trial. Circ Heart Fail. 2011;4(5):569–577. doi: 10.1161/CIRCHEARTFAILURE.111.962654. - DOI - PubMed
-
- Tschöpe C, Birner C, Böhm M, et al. Heart failure with preserved ejection fraction: current management and future strategies: expert opinion on the behalf of the nucleus of the “Heart Failure Working Group” of the German Society of Cardiology (DKG) Clin Res Cardiol. 2018;107:1–19. doi: 10.1007/s00392-017-1170-6. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
