

Progressive brain atrophy in chronically infected and treated HIV+ individuals
- PMID: 30767174
- PMCID: PMC6635004
- DOI: 10.1007/s13365-019-00723-4
Progressive brain atrophy in chronically infected and treated HIV+ individuals
Abstract
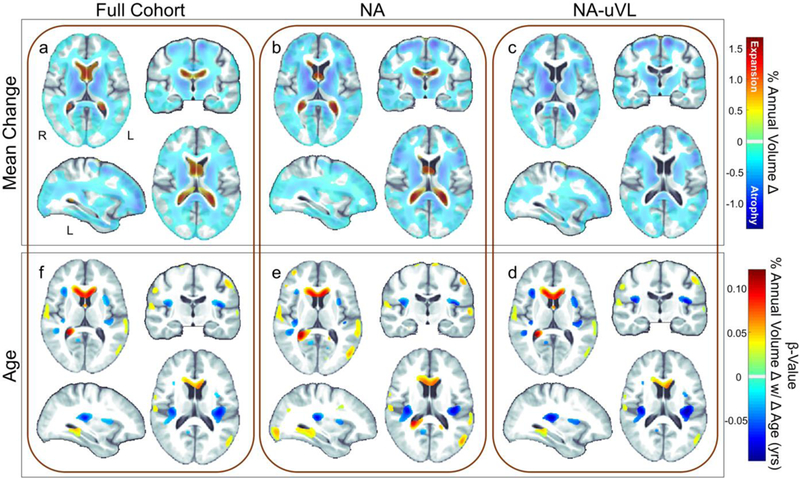
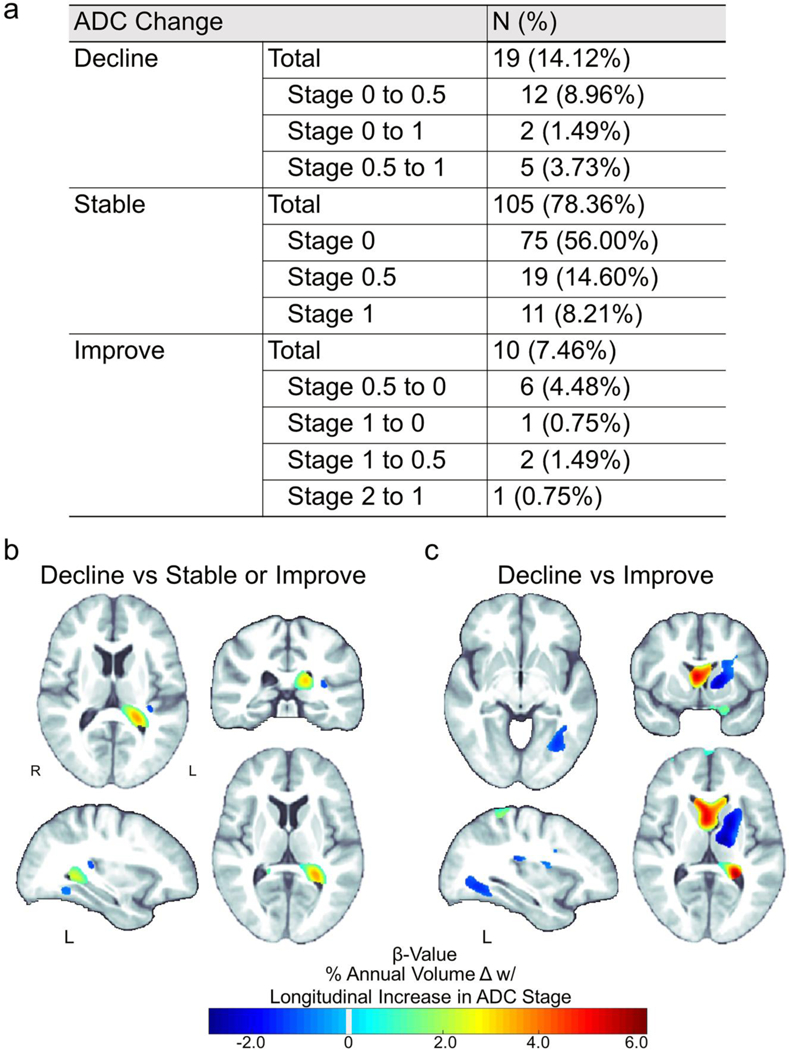
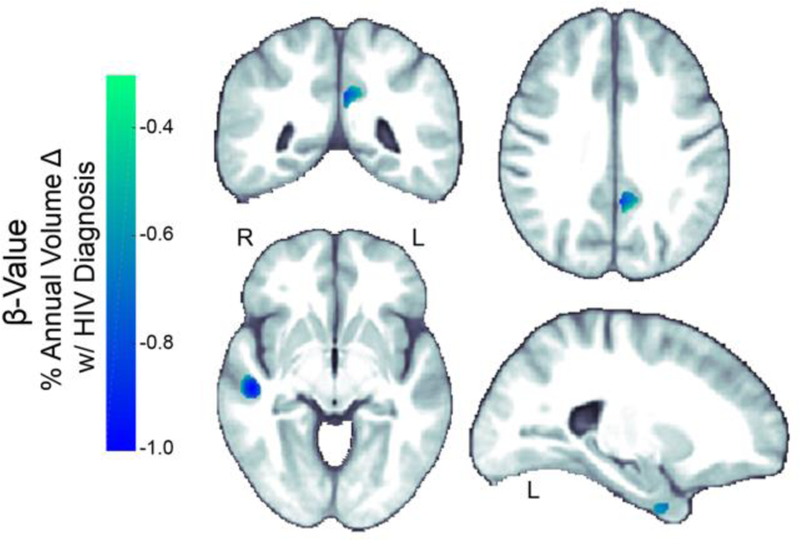
Growing evidence points to persistent neurological injury in chronic HIV infection. It remains unclear whether chronically HIV-infected individuals on combined antiretroviral therapy (cART) develop progressive brain injury and impaired neurocognitive function despite successful viral suppression and immunological restoration. In a longitudinal neuroimaging study for the HIV Neuroimaging Consortium (HIVNC), we used tensor-based morphometry to map the annual rate of change of regional brain volumes (mean time interval 1.0 ± 0.5 yrs), in 155 chronically infected and treated HIV+ participants (mean age 48.0 ± 8.9 years; 83.9% male) . We tested for associations between rates of brain tissue loss and clinical measures of infection severity (nadir or baseline CD4+ cell count and baseline HIV plasma RNA concentration), HIV duration, cART CNS penetration-effectiveness scores, age, as well as change in AIDS Dementia Complex stage. We found significant brain tissue loss across HIV+ participants, including those neuro-asymptomatic with undetectable viral loads, largely localized to subcortical regions. Measures of disease severity, age, and neurocognitive decline were associated with greater atrophy. Chronically HIV-infected and treated individuals may undergo progressive brain tissue loss despite stable and effective cART, which may contribute to neurocognitive decline. Understanding neurological complications of chronic infection and identifying factors associated with atrophy may help inform strategies to maintain brain health in people living with HIV.
Keywords: ADC; Brain volume; HIV; MRI; TBM; cART.
Conflict of interest statement
Conflict of Interest
Jeffry R Alger owns NeuroSpectroScopics LLC. Thomas B Campbell is a consultant for Gilead Sciences and Theratechnologies Inc. Xue Hua now works for M3 Biotechnology; the work included in the manuscript was conducted during her appointment at USC, and she reports no disclosures. The remaining authors declare that they have no conflict of interest.
Figures

References
-
- Ances BM and Ellis RJ (2007). Dementia and neurocognitive disorders due to HIV-1 infection. Semin Neurol, 27(1): 86–92. - PubMed
-
- Anderson AM, Harezlak J, Bharti A, Mi D, Taylor MJ, Daar ES, Schifitto G, Zhong J, Alger JR, Brown MS, Singer EJ, Campbell TB, McMahon DD, Buchthal S, Cohen R, Yiannoutsos C, Letendre SL, Navia BA and Consortium HIVN (2015). Plasma and Cerebrospinal Fluid Biomarkers Predict Cerebral Injury in HIV-Infected Individuals on Stable Combination Antiretroviral Therapy. J Acquir Immune Defic Syndr, 69(1): 29–35. - PMC - PubMed
-
- Antinori A, Arendt G, Becker JT, Brew BJ, Byrd DA, Cherner M, Clifford DB, Cinque P, Epstein LG, Goodkin K, Gisslen M, Grant I, Heaton RK, Joseph J, Marder K, Marra CM, McArthur JC, Nunn M, Price RW, Pulliam L, Robertson KR, Sacktor N, Valcour V and Wojna VE (2007). Updated research nosology for HIV-associated neurocognitive disorders. Neurology, 69(18): 1789–1799. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
