

Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals
- PMID: 30768188
- PMCID: PMC6484603
- DOI: 10.1001/jamanetworkopen.2018.7571
Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals
Abstract
Importance: Sepsis is present in many hospitalizations that culminate in death. The contribution of sepsis to these deaths, and the extent to which they are preventable, is unknown.
Objective: To estimate the prevalence, underlying causes, and preventability of sepsis-associated mortality in acute care hospitals.
Design, setting, and participants: Cohort study in which a retrospective medical record review was conducted of 568 randomly selected adults admitted to 6 US academic and community hospitals from January 1, 2014, to December 31, 2015, who died in the hospital or were discharged to hospice and not readmitted. Medical records were reviewed from January 1, 2017, to March 31, 2018.
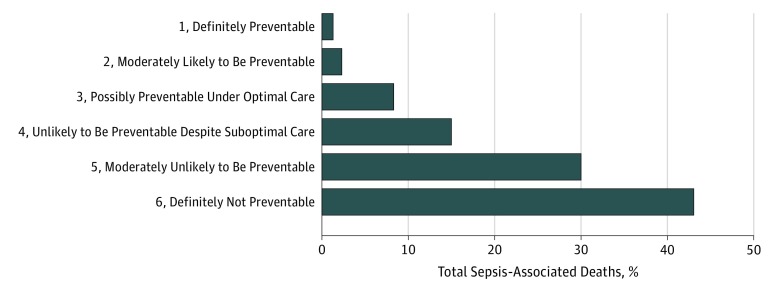
Main outcomes and measures: Clinicians reviewed cases for sepsis during hospitalization using Sepsis-3 criteria, hospice-qualifying criteria on admission, immediate and underlying causes of death, and suboptimal sepsis-related care such as inappropriate or delayed antibiotics, inadequate source control, or other medical errors. The preventability of each sepsis-associated death was rated on a 6-point Likert scale.
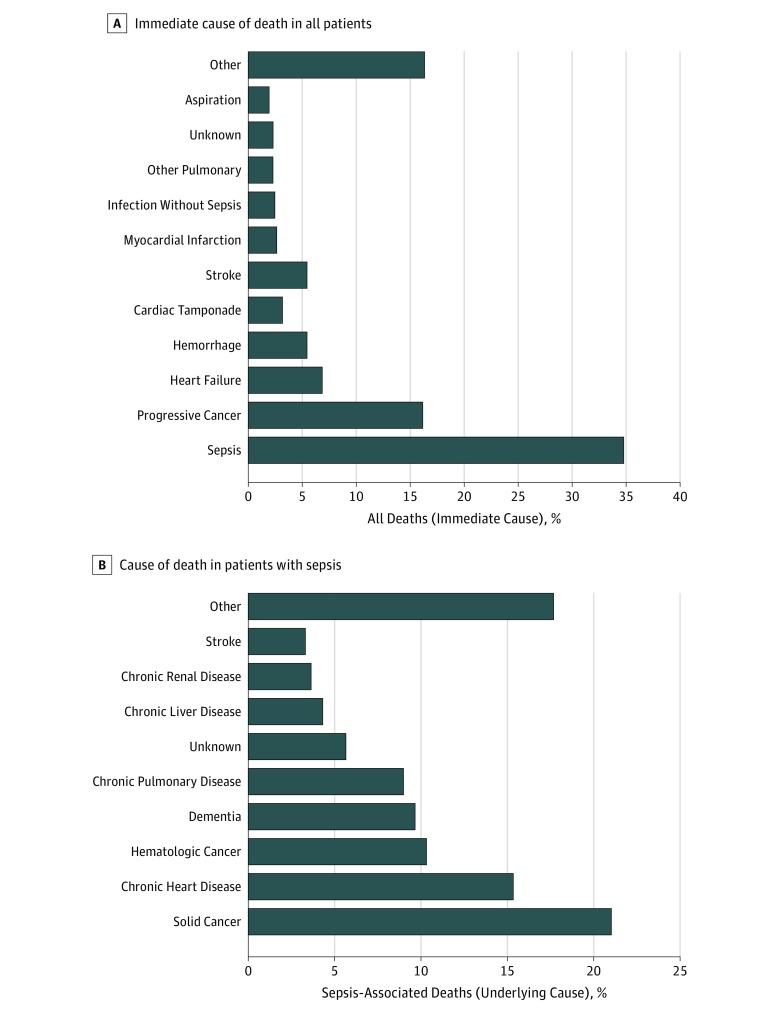
Results: The study cohort included 568 patients (289 [50.9%] men; mean [SD] age, 70.5 [16.1] years) who died in the hospital or were discharged to hospice. Sepsis was present in 300 hospitalizations (52.8%; 95% CI, 48.6%-57.0%) and was the immediate cause of death in 198 cases (34.9%; 95% CI, 30.9%-38.9%). The next most common immediate causes of death were progressive cancer (92 [16.2%]) and heart failure (39 [6.9%]). The most common underlying causes of death in patients with sepsis were solid cancer (63 of 300 [21.0%]), chronic heart disease (46 of 300 [15.3%]), hematologic cancer (31 of 300 [10.3%]), dementia (29 of 300 [9.7%]), and chronic lung disease (27 of 300 [9.0%]). Hospice-qualifying conditions were present on admission in 121 of 300 sepsis-associated deaths (40.3%; 95% CI 34.7%-46.1%), most commonly end-stage cancer. Suboptimal care, most commonly delays in antibiotics, was identified in 68 of 300 sepsis-associated deaths (22.7%). However, only 11 sepsis-associated deaths (3.7%) were judged definitely or moderately likely preventable; another 25 sepsis-associated deaths (8.3%) were considered possibly preventable.
Conclusions and relevance: In this cohort from 6 US hospitals, sepsis was the most common immediate cause of death. However, most underlying causes of death were related to severe chronic comorbidities and most sepsis-associated deaths were unlikely to be preventable through better hospital-based care. Further innovations in the prevention and care of underlying conditions may be necessary before a major reduction in sepsis-associated deaths can be achieved.
Conflict of interest statement
Figures
Comment in
-
A Closer Look at Sepsis-Associated Mortality.JAMA Netw Open. 2019 Feb 1;2(2):e187565. doi: 10.1001/jamanetworkopen.2018.7565. JAMA Netw Open. 2019. PMID: 30768185 No abstract available.
References
-
- Sepsis Alliance. Sepsis fact sheet. https://www.sepsis.org/downloads/2016_sepsis_facts_media.pdf. Accessed December 5, 2018.
-
- Martin GS, Mannino DM, Moss M. The effect of age on the development and outcome of adult sepsis. Crit Care Med. 2006;34(1):15-21. doi: 10.1097/01.CCM.0000194535.82812.BA - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
