

Organ Failure Due to Systemic Injury in Acute Pancreatitis
- PMID: 30768987
- PMCID: PMC6486861
- DOI: 10.1053/j.gastro.2018.12.041
Organ Failure Due to Systemic Injury in Acute Pancreatitis
Abstract
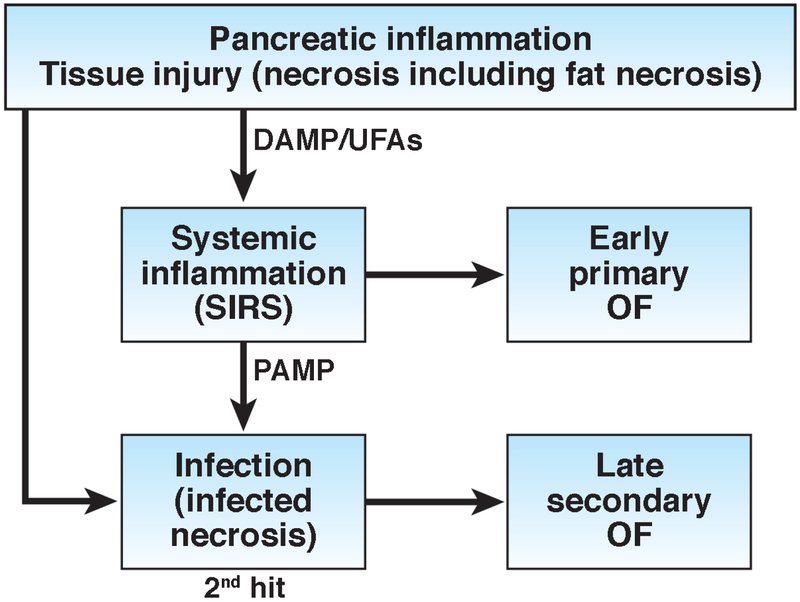
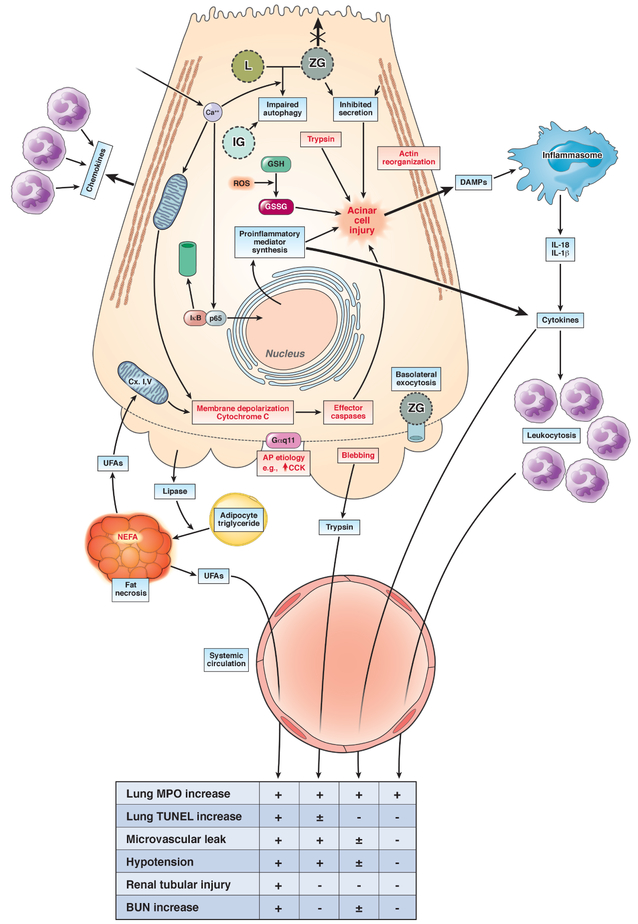
Acute pancreatitis may be associated with both local and systemic complications. Systemic injury manifests in the form of organ failure, which is seen in approximately 20% of all cases of acute pancreatitis and defines "severe acute pancreatitis." Organ failure typically develops early in the course of acute pancreatitis, but also may develop later due to infected pancreatic necrosis-induced sepsis. Organ failure is the most important determinant of outcome in acute pancreatitis. We review here the current understanding of the risk factors, pathophysiology, timing, impact on outcome, and therapy of organ failure in acute pancreatitis. As we discuss the pathophysiology of severe systemic injury, the distinctions between markers and mediators of severity are highlighted based on evidence supporting their causality in organ failure. Emphasis is placed on clinically relevant end points of organ failure and the mechanisms underlying the pathophysiological perturbations, which offer insight into potential therapeutic targets to treat.
Keywords: Acute Pancreatitis; Organ Failure; Pathophysiology.
Copyright © 2019 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Xiao AY, Tan ML, Wu LM, et al. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol 2016;1:45–55. - PubMed
-
- Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–11. - PubMed
-
- Garg PK, Madan K, Pande GK, et al. Association of extent and infection of pancreatic necrosis with organ failure and death in acute necrotizing pancreatitis. Clin Gastroenterol Hepatol 2005;3:159–66. - PubMed
-
- Mofidi R, Duff MD, Wigmore SJ, et al. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. The British journal of surgery 2006;93:738–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
