

Progressive Oncological Surgery Is Associated with Increased Curative Resection Rates and Improved Survival in Metastatic Colorectal Cancer
- PMID: 30769860
- PMCID: PMC6406820
- DOI: 10.3390/cancers11020218
Progressive Oncological Surgery Is Associated with Increased Curative Resection Rates and Improved Survival in Metastatic Colorectal Cancer
Abstract
Background: Secondary resection rates in first-line chemotherapy trials for metastatic colorectal cancer (mCRC) remain below 15%, representing a clear contrast to reports by specialised surgical centres, where progressive liver, peritoneal-surface, and pulmonary surgery increased access to curative-intent treatment. We present a long-term evaluation of oncosurgical management in a single-centre, analysing the aggregate effect of gradual implementation of surgical subspecialties and systemic treatments on mCRC patients' resection rates and prognosis.
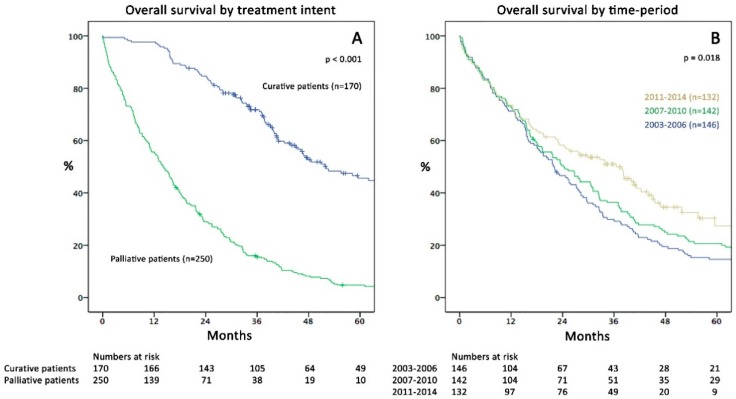
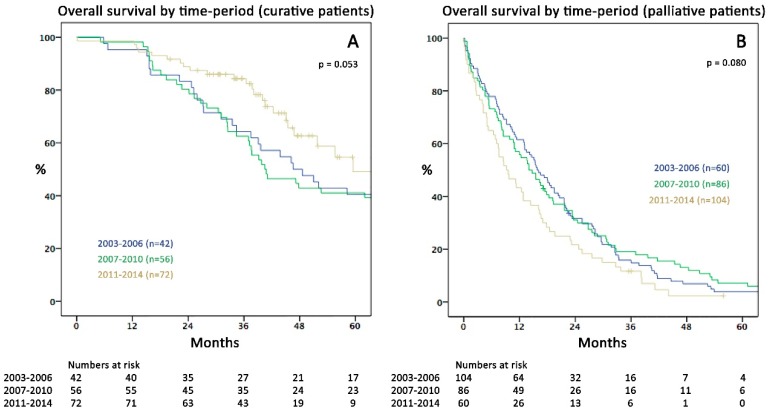
Methods: Patients with newly diagnosed mCRC from 2003 to 2014 were retrospectively categorised into palliative treatment (PAT) and curative intent surgery (CIS) and three time periods were analysed for treatment changes and factors associated with survival.
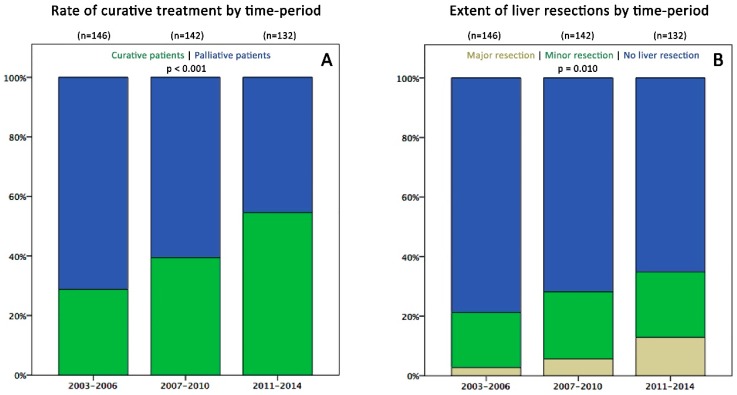
Results: Four hundred-twenty patients were treated (PAT:250/CIS:170). Over time periods, the number of presenting patients remained consistent, whereas curative resection rates increased from 29% to 55%, facilitated by an increment of patients undergoing hepatectomy (21 to 35%), pulmonary surgery (6 to 17%), and peritonectomy/intraoperative chemotherapy (0 to 8%). Also, recently, significantly more multi-line systemic treatments were applied. The median survival markedly improved from 21.9 months (2003⁻2006; 95% confidence interval (CI) 17.3⁻26.5) to 36.5 months (2011⁻2014; 95% CI 26.6⁻46.4; p = 0.018). PAT was a significant factor of poor survival and diagnosis of mCRC in the latest time period was independently associated with a distinctly lower risk for palliative treatment (odds ratio 0.15).
Conclusions: In modern eras of medical oncology, achieving appropriate resection rates through utilization of state-of-the-art oncological surgery by dedicated experts represents a cornerstone for long-term survival in mCRC.
Keywords: advances in management; colorectal cancer; curative intent; liver resection; metastases; modern chemotherapy; peritoneal surface surgery; pulmonary resection; resectability; surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gatta G., Capocaccia R., Sant M., Bell C.M., Coebergh J.W., Damhuis R.A., Faivre J., Martinez-Garcia C., Pawlega J., Ponz de Leon M., et al. Understanding variations in survival for colorectal cancer in europe: A eurocare high resolution study. Gut. 2000;47:533–538. doi: 10.1136/gut.47.4.533. - DOI - PMC - PubMed
-
- Mantke R., Schmidt U., Wolff S., Kube R., Lippert H. Incidence of synchronous liver metastases in patients with colorectal cancer in relationship to clinico-pathologic characteristics. Results of a german prospective multicentre observational study. Eur. J. Surg. Oncol. 2012;38:259–265. doi: 10.1016/j.ejso.2011.12.013. - DOI - PubMed
LinkOut - more resources
Full Text Sources
