

Increased Clinical Sensitivity and Specificity of Plasma Protein N-Glycan Profiling for Diagnosing Congenital Disorders of Glycosylation by Use of Flow Injection-Electrospray Ionization-Quadrupole Time-of-Flight Mass Spectrometry
- PMID: 30770376
- PMCID: PMC6886244
- DOI: 10.1373/clinchem.2018.296780
Increased Clinical Sensitivity and Specificity of Plasma Protein N-Glycan Profiling for Diagnosing Congenital Disorders of Glycosylation by Use of Flow Injection-Electrospray Ionization-Quadrupole Time-of-Flight Mass Spectrometry
Abstract
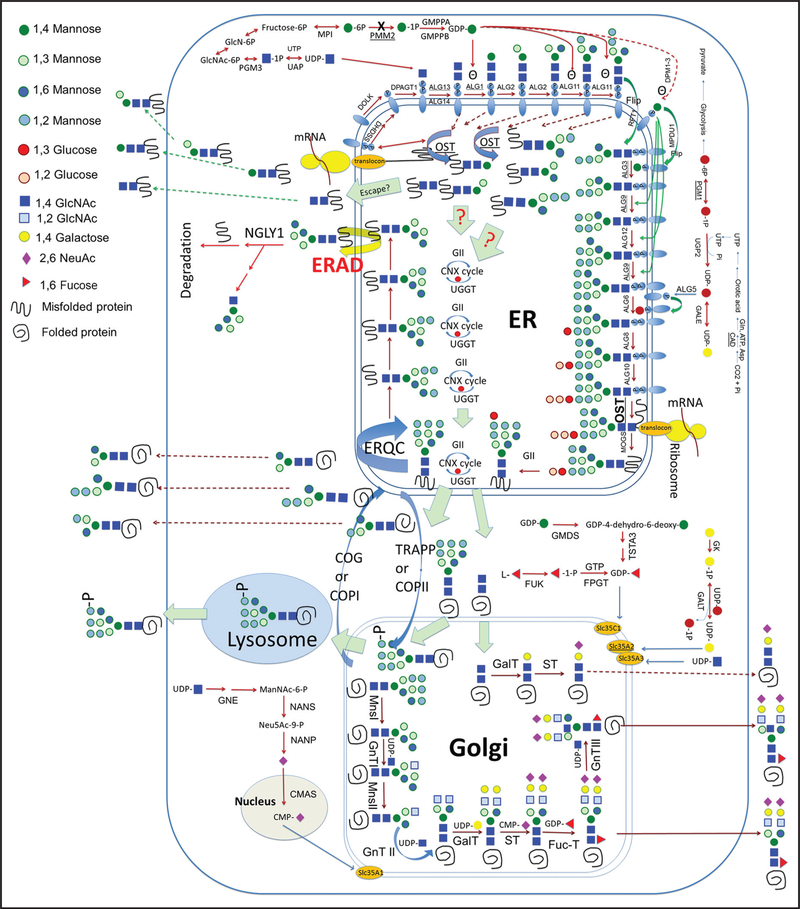
Background: Congenital disorders of glycosylation (CDG) represent 1 of the largest groups of metabolic disorders with >130 subtypes identified to date. The majority of CDG subtypes are disorders of N-linked glycosylation, in which carbohydrate residues, namely, N-glycans, are posttranslationally linked to asparagine molecules in peptides. To improve the diagnostic capability for CDG, we developed and validated a plasma N-glycan assay using flow injection-electrospray ionization-quadrupole time-of-flight mass spectrometry.
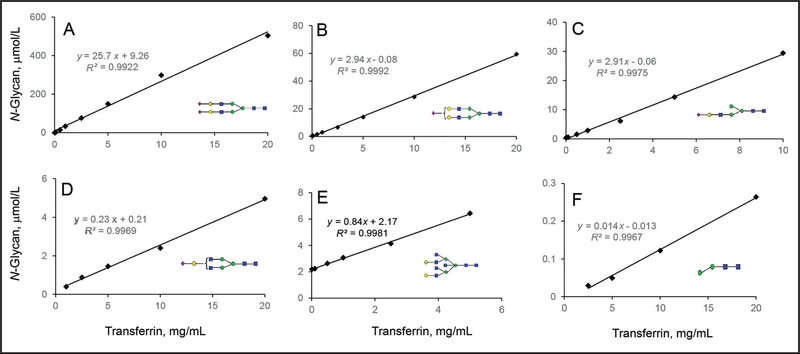
Methods: After PNGase F digestion of plasma glycoproteins, N-glycans were linked to a quinolone using a transient amine group at the reducing end, isolated by a hydrophilic interaction chromatography column, and then identified by accurate mass and quantified using a stable isotope-labeled glycopeptide as the internal standard.
Results: This assay differed from other N-glycan profiling methods because it was free of any contamination from circulating free glycans and was semiquantitative. The low end of the detection range tested was at 63 nmol/L for disialo-biantennary N-glycan. The majority of N-glycans in normal plasma had <1% abundance. Abnormal N-glycan profiles from 19 patients with known diagnoses of 11 different CDG subtypes were generated, some of which had previously been reported to have normal N-linked protein glycosylation by carbohydrate-deficient transferrin analysis.
Conclusions: The clinical specificity and sensitivity of N-glycan analysis was much improved with this method. Additional CDGs can be diagnosed that would be missed by carbohydrate-deficient transferrin analysis. The assay provides novel biomarkers with diagnostic and potentially therapeutic significance.
© 2019 American Association for Clinical Chemistry.
Conflict of interest statement
Figures


Comment in
-
Improving biochemical markers for disorders of N-glycosylation.Ann Transl Med. 2019 Sep;7(Suppl 6):S176. doi: 10.21037/atm.2019.07.79. Ann Transl Med. 2019. PMID: 31656755 Free PMC article. No abstract available.
-
Clinical glycomics in the diagnostic laboratory.Ann Transl Med. 2019 Sep;7(Suppl 6):S220. doi: 10.21037/atm.2019.08.74. Ann Transl Med. 2019. PMID: 31656799 Free PMC article. No abstract available.
-
Integrating mass spectrometry-based plasma (or serum) protein N-glycan profiling into the clinical practice?Ann Transl Med. 2019 Sep;7(Suppl 6):S225. doi: 10.21037/atm.2019.08.04. Ann Transl Med. 2019. PMID: 31656804 Free PMC article. No abstract available.
References
-
- Peanne R, de Lonlay P, Foulquier F, Kornak U, Lefeber DJ, Morava E, et al. Congenital disorders of glycosylation (CDG): quo vadis? Eur J Med Genet 2018;61:643–63. - PubMed
-
- Xia B, Zhang W, Li X, Jiang R, Harper T, Liu R, et al. Serum N-glycan and O-glycan analysis by mass spectrometry for diagnosis of congenital disorders of glycosylation. Anal Biochem 2013;442:178–85. - PubMed
-
- Saldova R, Stockmann H, O’Flaherty R, Lefeber DJ, Jaeken J, Rudd PM. N-Glycosylation of serum IgG and total glycoproteins in MAN1B1 deficiency. J Proteome Res 2015;14:4402–12. - PubMed
