

Mortality after breast cancer as a function of time since diagnosis by estrogen receptor status and age at diagnosis
- PMID: 30771221
- PMCID: PMC6697632
- DOI: 10.1002/ijc.32214
Mortality after breast cancer as a function of time since diagnosis by estrogen receptor status and age at diagnosis
Abstract
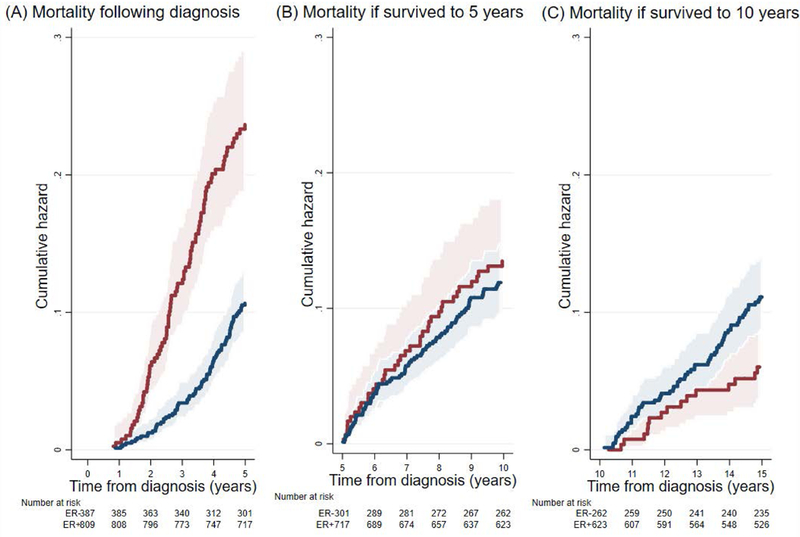
Our aim was to estimate how long-term mortality following breast cancer diagnosis depends on age at diagnosis, tumor estrogen receptor (ER) status, and the time already survived. We used the population-based Australian Breast Cancer Family Study which followed-up 1,196 women enrolled during 1992-1999 when aged <60 years at diagnosis with a first primary invasive breast cancer, over-sampled for younger ages at diagnosis, for whom tumor pathology features and ER status were measured. There were 375 deaths (median follow-up = 15.7; range = 0.8-21.4, years). We estimated the mortality hazard as a function of time since diagnosis using a flexible parametric survival analysis with ER status a time-dependent covariate. For women with ER-negative tumors compared with those with ER-positive tumors, 5-year mortality was initially higher (p < 0.001), similar if they survived to 5 years (p = 0.4), and lower if they survived to 10 years (p = 0.02). The estimated mortality hazard for ER-negative disease peaked at ~3 years post-diagnosis, thereafter declined with time, and at 7 years post-diagnosis became lower than that for ER-positive disease. This pattern was more pronounced for women diagnosed at younger ages. Mortality was also associated with lymph node count (hazard ratio (HR) per 10 nodes = 2.52 [95% CI:2.11-3.01]) and tumor grade (HR per grade = 1.62 [95% CI:1.34-1.96]). The risk of death following a breast cancer diagnosis differs substantially and qualitatively with diagnosis age, ER status and time survived. For women who survive >7 years, those with ER-negative disease will on average live longer, and more so if younger at diagnosis.
Keywords: breast cancer; cohort study; estrogen receptor; mortality; survival; time-dependent effects.
© 2019 UICC.
Conflict of interest statement
Figures


References
-
- Anders CK, Hsu DS, Broadwater G, et al. Young age at diagnosis correlates with worse prognosis and defines a subset of breast cancers with shared patterns of gene expression. J Clin Oncol 2008; 26(20): 3324–3330. - PubMed
-
- Goldhirsch A, Glick JH, Gelber RD, et al. Meeting highlights: international expert consensus on the primary therapy of early breast cancer 2005. Ann Oncol 2005; 16(10): 1569–1583. - PubMed
-
- Copson E, Eccles B, Maishman T, et al. Prospective observational study of breast cancer treatment outcomes for UK women aged 18–40 years at diagnosis: the POSH study. J Natl Cancer Inst 2013; 105(13): 978–988. - PubMed
-
- Bentzon N, During M, Rasmussen BB, et al. Prognostic effect of estrogen receptor status across age in primary breast cancer. Int J Cancer 2008; 122(5): 1089–1094. - PubMed
-
- Liukkonen S, Leidenius M, Saarto T, et al. Breast cancer in very young women. Eu J Surg Oncol 2011; 37(12): 1030–1037. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
