

Therapist-guided and parent-guided internet-delivered behaviour therapy for paediatric Tourette's disorder: a pilot randomised controlled trial with long-term follow-up
- PMID: 30772854
- PMCID: PMC6398666
- DOI: 10.1136/bmjopen-2018-024685
Therapist-guided and parent-guided internet-delivered behaviour therapy for paediatric Tourette's disorder: a pilot randomised controlled trial with long-term follow-up
Abstract
Objective: Behaviour therapy (BT) for Tourette's disorder (TD) and persistent (chronic) motor or vocal tic disorder (PTD) is rarely available. We evaluated the feasibility of adapting two existing BT protocols for TD/PTD (habit reversal training (HRT) and exposure and response prevention (ERP)) into a therapist-guided and parent-guided online self-help format.
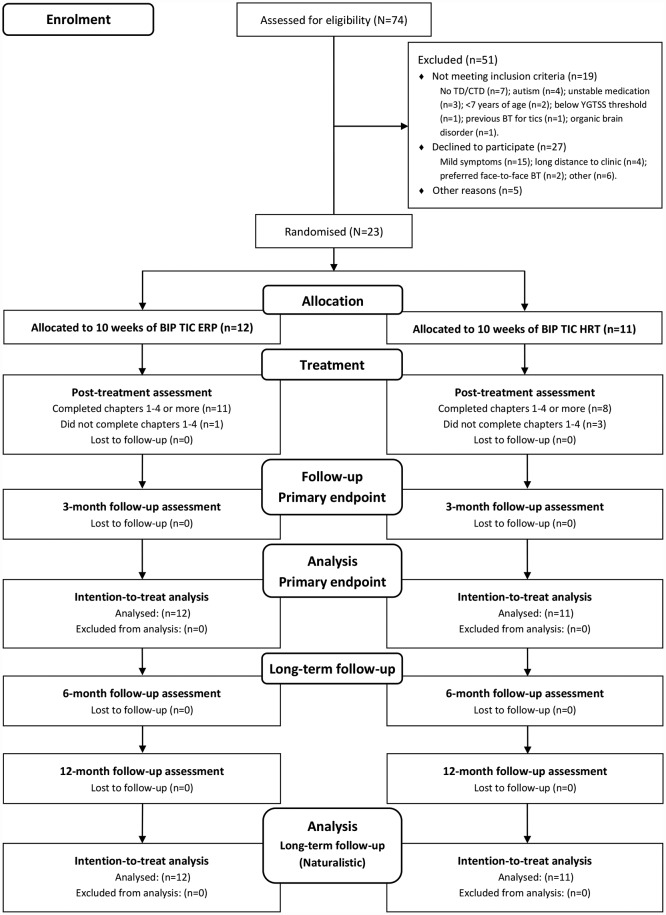
Design: A pilot, single-blind, parallel group randomised controlled trial.
Setting: A specialist outpatient clinic in Sweden.
Participants: Twenty-three young people with TD/PTD, aged 8-16.
Interventions: Two 10-week therapist-guided and parent-guided internet-delivered programmes (called BIP TIC HRT and BIP TIC ERP).
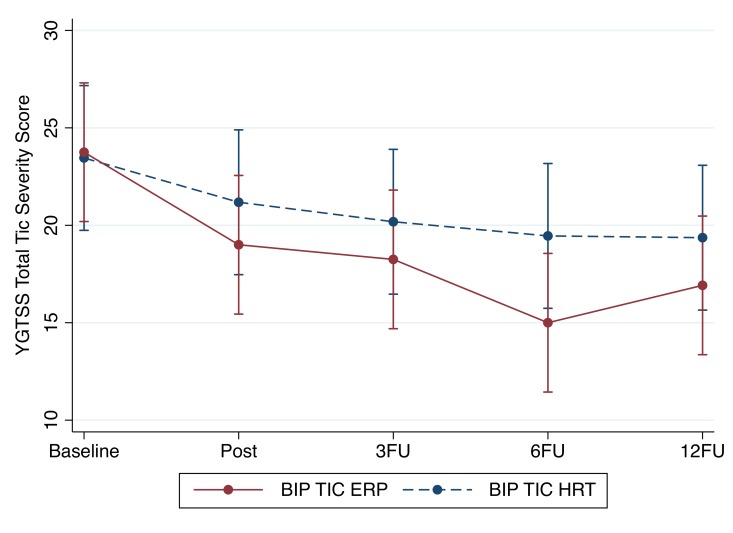
Outcome: The primary outcome measure was the Yale Global Tic Severity Scale. Blinded evaluators rated symptoms at baseline, post-treatment and 3-month follow-up (primary endpoint). All participants were naturalistically followed up to 12 months after treatment.
Results: Patients and parents rated the interventions as highly acceptable, credible and satisfactory. While both interventions resulted in reduced tic-related impairment, parent-rated tic severity and improved quality of life, only BIP TIC ERP resulted in a significant improvement on the primary outcome measure. Within-group effect sizes and responder rates were, respectively: d=1.12 and 75% for BIP TIC ERP, and d=0.50 and 55% for BIP TIC HRT. The therapeutic gains were maintained up to 12 months after the end of the treatment. Adverse events were rare in both groups. The average therapist support time was around 25 min per participant per week.
Conclusions: Internet-delivered BT has the potential to greatly increase access to evidence-based treatment for young people with TD/PTD. Further evaluation of the efficacy and cost-effectiveness of this treatment modality is warranted.
Trial registration number: NCT02864589; Pre-results.
Keywords: Tourette’s disorder; behaviour therapy; persistent (chronic) motor or vocal tic disorder; telemedicine.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: LFC and DM-C receive royalties for contributing articles to UpToDate, Wolters Kluwer Health.
Figures
References
-
- Hollis C, Pennant M, Cuenca J, et al. . Clinical effectiveness and patient perspectives of different treatment strategies for tics in children and adolescents with Tourette syndrome: a systematic review and qualitative analysis. Health Technol Assess 2016;20:1–450. 10.3310/hta20040 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical