

Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial
- PMID: 30772908
- PMCID: PMC6439620
- DOI: 10.1001/jama.2019.0071
Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial
Abstract
Importance: Abnormal peripheral perfusion after septic shock resuscitation has been associated with organ dysfunction and mortality. The potential role of the clinical assessment of peripheral perfusion as a target during resuscitation in early septic shock has not been established.
Objective: To determine if a peripheral perfusion-targeted resuscitation during early septic shock in adults is more effective than a lactate level-targeted resuscitation for reducing mortality.
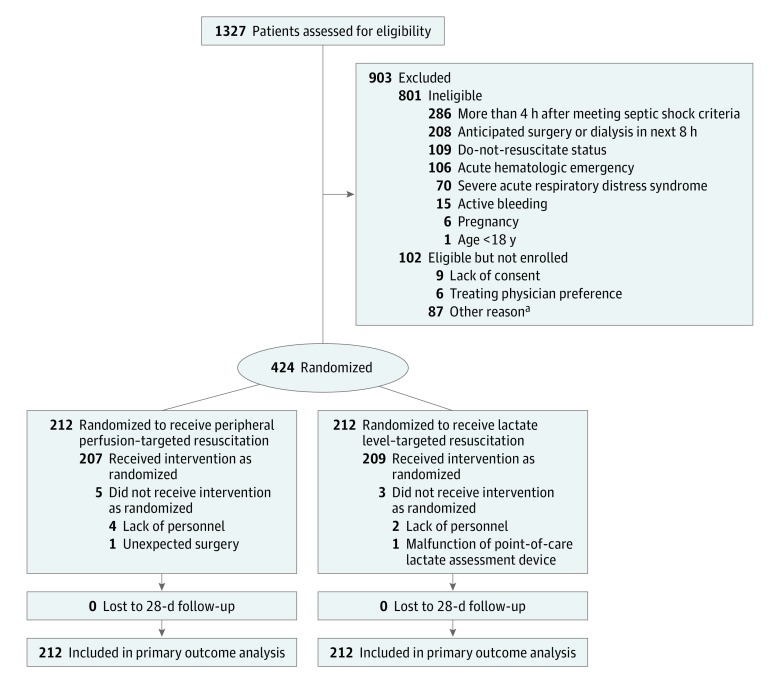
Design, setting, and participants: Multicenter, randomized trial conducted at 28 intensive care units in 5 countries. Four-hundred twenty-four patients with septic shock were included between March 2017 and March 2018. The last date of follow-up was June 12, 2018.
Interventions: Patients were randomized to a step-by-step resuscitation protocol aimed at either normalizing capillary refill time (n = 212) or normalizing or decreasing lactate levels at rates greater than 20% per 2 hours (n = 212), during an 8-hour intervention period.
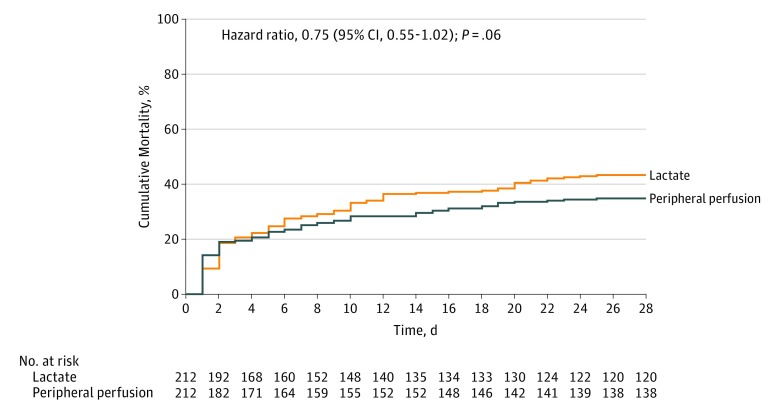
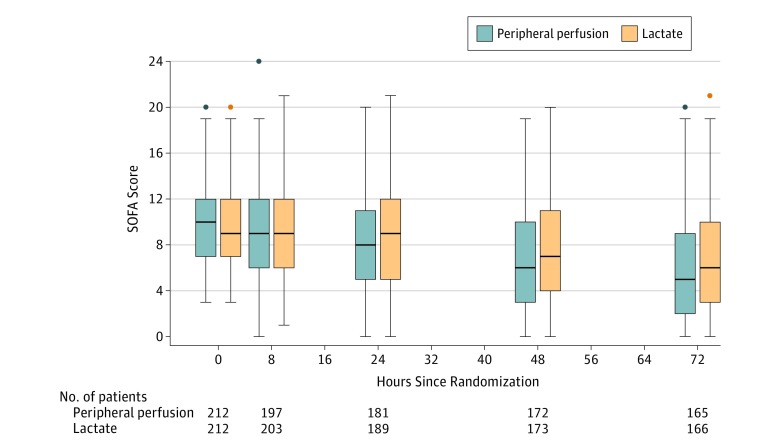
Main outcomes and measures: The primary outcome was all-cause mortality at 28 days. Secondary outcomes were organ dysfunction at 72 hours after randomization, as assessed by Sequential Organ Failure Assessment (SOFA) score (range, 0 [best] to 24 [worst]); death within 90 days; mechanical ventilation-, renal replacement therapy-, and vasopressor-free days within 28 days; intensive care unit and hospital length of stay.
Results: Among 424 patients randomized (mean age, 63 years; 226 [53%] women), 416 (98%) completed the trial. By day 28, 74 patients (34.9%) in the peripheral perfusion group and 92 patients (43.4%) in the lactate group had died (hazard ratio, 0.75 [95% CI, 0.55 to 1.02]; P = .06; risk difference, -8.5% [95% CI, -18.2% to 1.2%]). Peripheral perfusion-targeted resuscitation was associated with less organ dysfunction at 72 hours (mean SOFA score, 5.6 [SD, 4.3] vs 6.6 [SD, 4.7]; mean difference, -1.00 [95% CI, -1.97 to -0.02]; P = .045). There were no significant differences in the other 6 secondary outcomes. No protocol-related serious adverse reactions were confirmed.
Conclusions and relevance: Among patients with septic shock, a resuscitation strategy targeting normalization of capillary refill time, compared with a strategy targeting serum lactate levels, did not reduce all-cause 28-day mortality.
Trial registration: ClinicalTrials.gov Identifier: NCT03078712.
Conflict of interest statement
Figures
Comment in
-
How Best to Resuscitate Patients With Septic Shock?JAMA. 2019 Feb 19;321(7):647-648. doi: 10.1001/jama.2019.0070. JAMA. 2019. PMID: 30772916 No abstract available.
-
Strategy focused on clinical parameters of microcirculation to resuscitate patients in septic shock: Do not forget any tools.Anaesth Crit Care Pain Med. 2019 Jun;38(3):209-210. doi: 10.1016/j.accpm.2019.04.011. Anaesth Crit Care Pain Med. 2019. PMID: 31076140 No abstract available.
-
Lactate-Guided Resuscitation Strategies in Septic Shock: Differentiating the Bad From the Unexceptional: June 2019 Annals of Emergency Medicine Journal Club.Ann Emerg Med. 2019 Jun;73(6):688-690. doi: 10.1016/j.annemergmed.2019.04.010. Ann Emerg Med. 2019. PMID: 31133184 No abstract available.
-
Resuscitation Strategies Using Peripheral Perfusion vs Serum Lactate Levels.JAMA. 2019 Jul 9;322(2):172. doi: 10.1001/jama.2019.6027. JAMA. 2019. PMID: 31287517 No abstract available.
-
Resuscitation Strategies Using Peripheral Perfusion vs Serum Lactate Levels.JAMA. 2019 Jul 9;322(2):172-173. doi: 10.1001/jama.2019.6031. JAMA. 2019. PMID: 31287518 No abstract available.
-
Targeting peripheral perfusion versus serum lactate levels in septic shock.Intern Emerg Med. 2019 Sep;14(6):999-1001. doi: 10.1007/s11739-019-02152-x. Epub 2019 Jul 18. Intern Emerg Med. 2019. PMID: 31321708 No abstract available.
-
Lactate guided resuscitation-nothing is more dangerous than conscientious foolishness.J Thorac Dis. 2019 Sep;11(Suppl 15):S1969-S1972. doi: 10.21037/jtd.2019.07.67. J Thorac Dis. 2019. PMID: 31632800 Free PMC article. No abstract available.
-
Basics of changes in hemodynamic monitoring in sepsis care.J Thorac Dis. 2019 Oct;11(10):E168-E170. doi: 10.21037/jtd.2019.09.43. J Thorac Dis. 2019. PMID: 31737330 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
