

Population genomic screening of all young adults in a health-care system: a cost-effectiveness analysis
- PMID: 30773532
- PMCID: PMC6752319
- DOI: 10.1038/s41436-019-0457-6
Population genomic screening of all young adults in a health-care system: a cost-effectiveness analysis
Erratum in
-
Correction: Population genomic screening of all young adults in a health-care system: a cost-effectiveness analysis.Genet Med. 2019 Sep;21(9):2162-2163. doi: 10.1038/s41436-019-0515-0. Genet Med. 2019. PMID: 30944416 Free PMC article.
Abstract
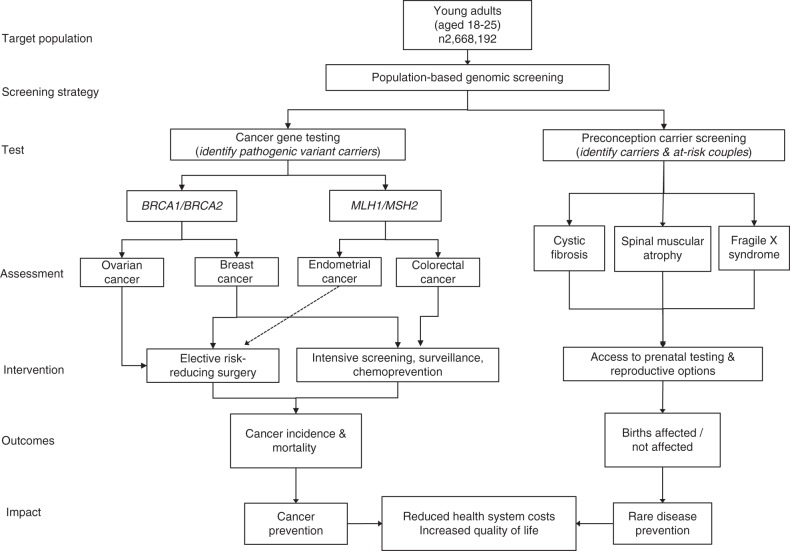
Purpose: To consider the impact and cost-effectiveness of offering preventive population genomic screening to all young adults in a single-payer health-care system.
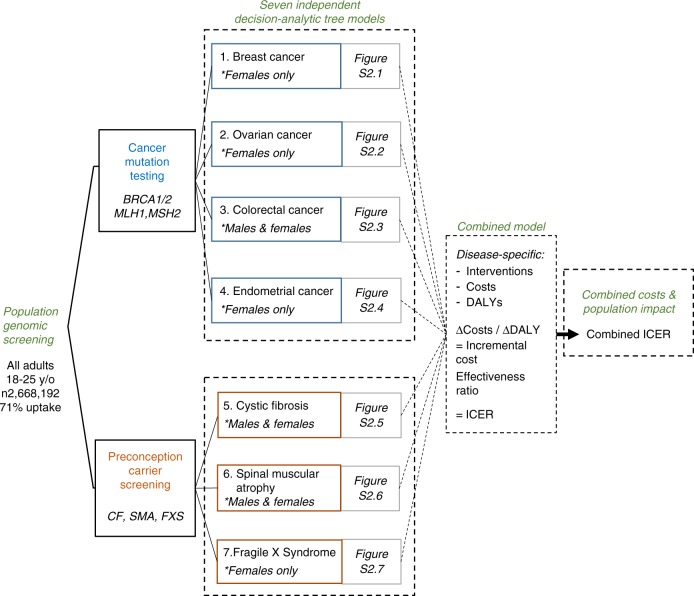
Methods: We modeled screening of 2,688,192 individuals, all adults aged 18-25 years in Australia, for pathogenic variants in BRCA1/BRCA2/MLH1/MSH2 genes, and carrier screening for cystic fibrosis (CF), spinal muscular atrophy (SMA), and fragile X syndrome (FXS), at 71% testing uptake using per-test costs ranging from AUD$200 to $1200 (~USD$140 to $850). Investment costs included genetic counseling, surveillance, and interventions (reimbursed only) for at-risk individuals/couples. Cost-effectiveness was defined below AUD$50,000/DALY (disability-adjusted life year) prevented, using an incremental cost-effectiveness ratio (ICER), compared with current targeted testing. Outcomes were cancer incidence/mortality, disease cases, and treatment costs reduced.
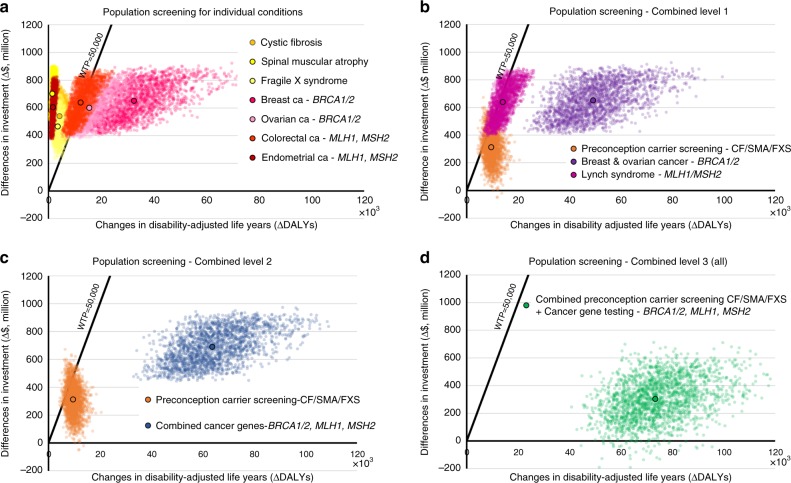
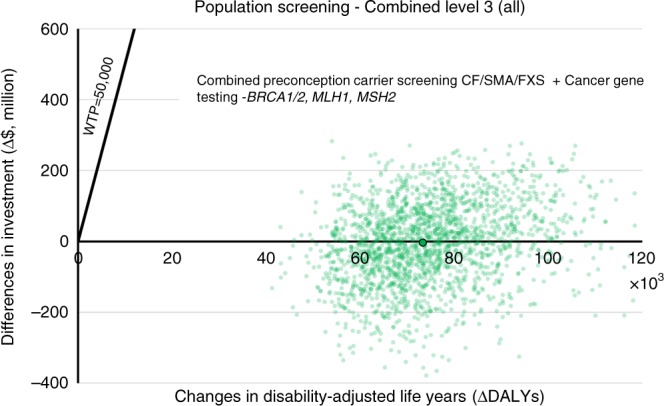
Results: Population screening would reduce variant-attributable cancers by 28.8%, cancer deaths by 31.2%, and CF/SMA/FXS cases by 24.8%, compared with targeted testing. Assuming AUD$400 per test, investment required would be between 4 and 5 times higher than current expenditure. However, screening would lead to substantial savings in medical costs and DALYs prevented, at a highly cost-effective ICER of AUD$4038/DALY. At AUD$200 per test, screening would approach cost-saving for the health system (ICER = AUD$22/DALY).
Conclusion: Preventive genomic screening in early adulthood would be highly cost-effective in a single-payer health-care system, but ethical issues must be considered.
Keywords: cancer; cost-effectiveness analysis; population genomic screening; preconception carrier screening; prevention.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Cost-effectiveness of population genomic screening.Genet Med. 2019 Dec;21(12):2840-2841. doi: 10.1038/s41436-019-0580-4. Genet Med. 2019. PMID: 31303645 No abstract available.
-
Response to Veenstra et al.Genet Med. 2019 Dec;21(12):2842-2843. doi: 10.1038/s41436-019-0581-3. Epub 2019 Jul 15. Genet Med. 2019. PMID: 31303646 No abstract available.
References
-
- Alver M, Palover M, Saar A, et al. Recall by genotype and cascade screening for familial hypercholesterolemia in a population-based biobank from Estonia. Genet Med. 2018 Oct 1; 10.1038/s41436-018-0311-2 [Epub ahead of print]. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
