

Statin use and prognosis of lung cancer: a systematic review and meta-analysis of observational studies and randomized controlled trials
- PMID: 30774306
- PMCID: PMC6350654
- DOI: 10.2147/DDDT.S187690
Statin use and prognosis of lung cancer: a systematic review and meta-analysis of observational studies and randomized controlled trials
Abstract
Background: Previous clinical studies reported inconsistent results on the associations of statins with the mortality and survival of lung cancer patients. This review and meta-analysis summarized the impact of statins on mortality and survival of lung cancer patients.
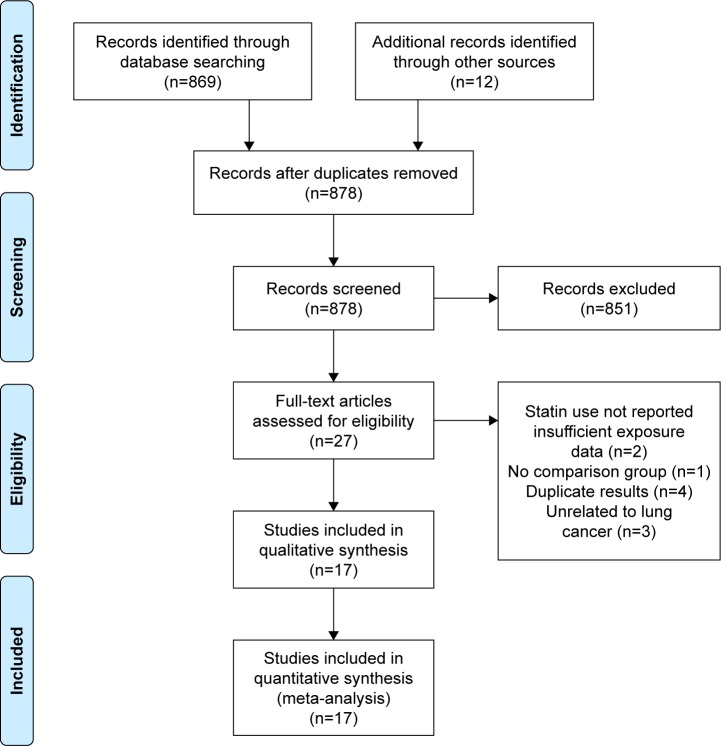
Materials and methods: Eligible papers of this meta-analysis were searched by using PubMed, EMBASE, and Cochrane until July 2017. Primary end points were the mortality (all-cause mortality and cancer-specific mortality) and survival (progression-free survival and overall survival) of patients with statin use. Secondary end points were overall response rate and safety. The random-effects model was used to calculate pooled HRs and 95% CIs.
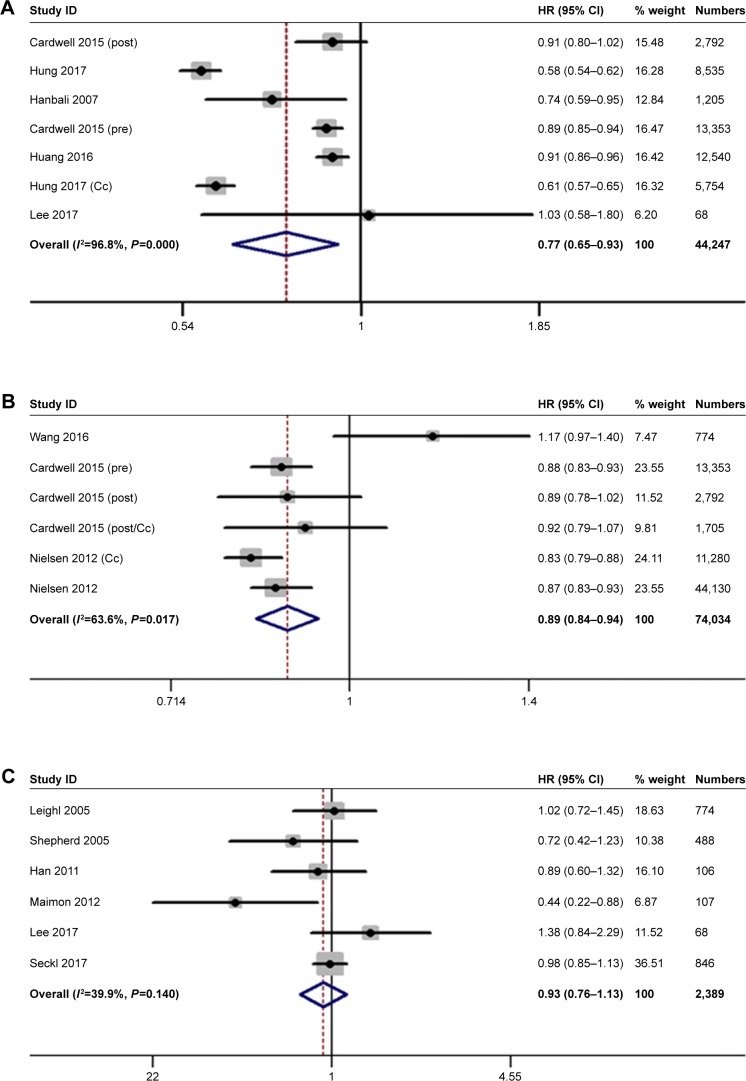
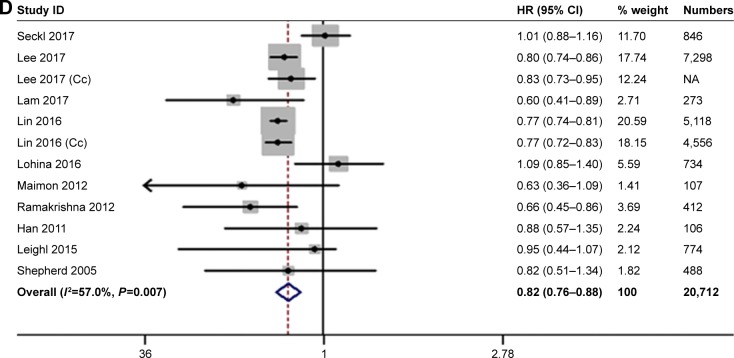
Results: Seventeen studies involving 98,445 patients were included in the meta-analysis. In observational studies, the pooled HR indicated that statins potentially decreased the cancer-specific mortality and promoted the overall survival of lung cancer patients. Statins showed an association with decreased all-cause mortality in cohort studies (HR =0.77, 95% CI: 0.59-0.99), but not in case-control studies (HR =0.75, 95% CI: 0.50-1.10). However, statin use showed no impact on mortality and overall survival in randomized controlled trials. Meanwhile, this meta-analysis indicated that statin use did not affect the progression-free survival of lung cancer patients in observational studies and randomized controlled trials. In addition, statins potentially enhanced the effects of tyrosine kinase inhibitors (HR=0.86, 95% CI: 0.76-0.98) and chemotherapy (HR=0.86, 95% CI: 0.81-0.91) on the overall survival of patients with non-small-cell lung cancer, but did not increase overall response rate and toxicity.
Conclusion: Statins were potentially associated with the decreasing risk of mortality and the improvement of overall survival in observational studies but not in randomized controlled trials.
Keywords: lung cancer; mortality; prognosis; statin; statins; survival.
Conflict of interest statement
Disclosure The authors report no conflicts of interests in this work.
Figures
Similar articles
-
Effects of statin exposure and lung cancer survival: A meta-analysis of observational studies.Pharmacol Res. 2019 Mar;141:357-365. doi: 10.1016/j.phrs.2019.01.016. Epub 2019 Jan 11. Pharmacol Res. 2019. PMID: 30641276
-
Statin therapy in the treatment of active cancer: A systematic review and meta-analysis of randomized controlled trials.PLoS One. 2018 Dec 20;13(12):e0209486. doi: 10.1371/journal.pone.0209486. eCollection 2018. PLoS One. 2018. PMID: 30571754 Free PMC article.
-
Impact of statin use on cancer-specific mortality and recurrence: A meta-analysis of 60 observational studies.Medicine (Baltimore). 2020 Apr;99(14):e19596. doi: 10.1097/MD.0000000000019596. Medicine (Baltimore). 2020. PMID: 32243380 Free PMC article.
-
Association of statin use in older people primary prevention group with risk of cardiovascular events and mortality: a systematic review and meta-analysis of observational studies.BMC Med. 2021 Jun 22;19(1):139. doi: 10.1186/s12916-021-02009-1. BMC Med. 2021. PMID: 34154589 Free PMC article.
-
Statin use improves survival in patients with pancreatic ductal adenocarcinoma: A meta-analysis.Dig Liver Dis. 2020 Apr;52(4):392-399. doi: 10.1016/j.dld.2020.01.008. Epub 2020 Feb 27. Dig Liver Dis. 2020. PMID: 32113888
Cited by
-
Beta Blockers with Statins May Decrease All-Cause Mortality in Patients with Cardiovascular Diseases and Locally Advanced Unresectable Non-Small-Cell Lung Cancer after Chemoradiotherapy.Cancers (Basel). 2023 Feb 17;15(4):1277. doi: 10.3390/cancers15041277. Cancers (Basel). 2023. PMID: 36831618 Free PMC article.
-
Survival Benefit of Statin with Anti-Angiogenesis Efficacy in Lung Cancer-Associated Pleural Fluid through FXR Modulation.Cancers (Basel). 2022 Jun 2;14(11):2765. doi: 10.3390/cancers14112765. Cancers (Basel). 2022. PMID: 35681743 Free PMC article.
-
Statin use after cancer diagnosis and survival among patients with cancer.Cancer Causes Control. 2025 Apr;36(4):443-455. doi: 10.1007/s10552-024-01939-4. Epub 2024 Dec 25. Cancer Causes Control. 2025. PMID: 39719543
-
Mutant p53, the Mevalonate Pathway and the Tumor Microenvironment Regulate Tumor Response to Statin Therapy.Cancers (Basel). 2022 Jul 19;14(14):3500. doi: 10.3390/cancers14143500. Cancers (Basel). 2022. PMID: 35884561 Free PMC article. Review.
-
[Research Progress on the Relationship between Blood Lipids and Lung Cancer Risk and Prognosis].Zhongguo Fei Ai Za Zhi. 2020 Sep 20;23(9):824-829. doi: 10.3779/j.issn.1009-3419.2020.102.36. Epub 2020 Aug 10. Zhongguo Fei Ai Za Zhi. 2020. PMID: 32773011 Free PMC article. Review. Chinese.
References
-
- Lee YG, Lee JH, Jang JS, Kim JH. Prognostic benefit of statin with or without metformin in elderly patients with advanced non-small cell lung cancer: a nationwide population-based outcome study. J Clin Oncol. 2017;35(15_suppl):e20661.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
