

Pharmacological interventions for the prevention of contrast-induced acute kidney injury in high-risk adult patients undergoing coronary angiography: a systematic review and meta-analysis of randomised controlled trials
- PMID: 30774964
- PMCID: PMC6350720
- DOI: 10.1136/openhrt-2018-000864
Pharmacological interventions for the prevention of contrast-induced acute kidney injury in high-risk adult patients undergoing coronary angiography: a systematic review and meta-analysis of randomised controlled trials
Abstract
Objective: Quantify the efficacy of strategies to prevent contrast-induced acute kidney injury (CI-AKI) in high-risk patients undergoing coronary angiography (CAG) with or without percutaneous coronary intervention (PCI).
Background: CI-AKI remains a common problem. The renoprotective efficacy of existing pharmacological agents remains uncertain in high-risk populations.
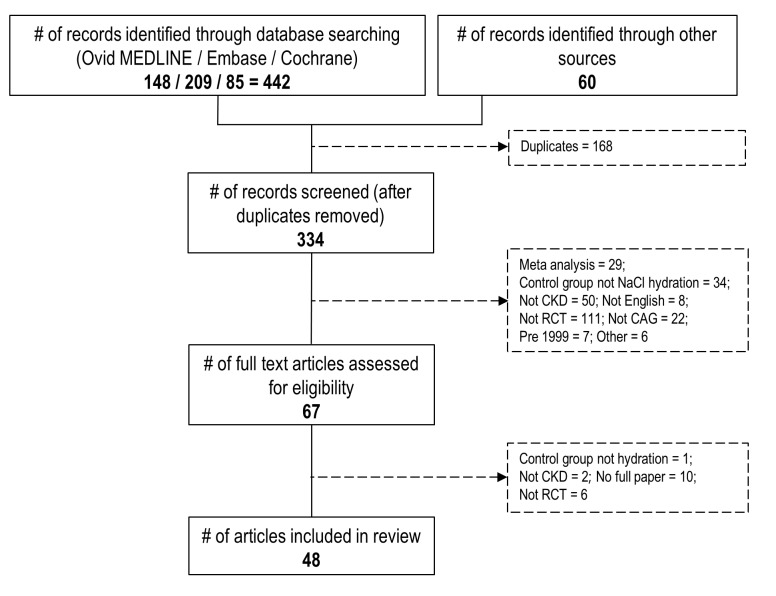
Methods: Systematic review and meta-analysis of randomised controlled trials (RCTs) to compare different strategies versus hydration in patients with chronic kidney disease (CKD) undergoing CAG±PCI. Primary outcome was incident CI-AKI. Fixed-effects meta-analyses estimated ORs, 95% CIs and heterogeneity.
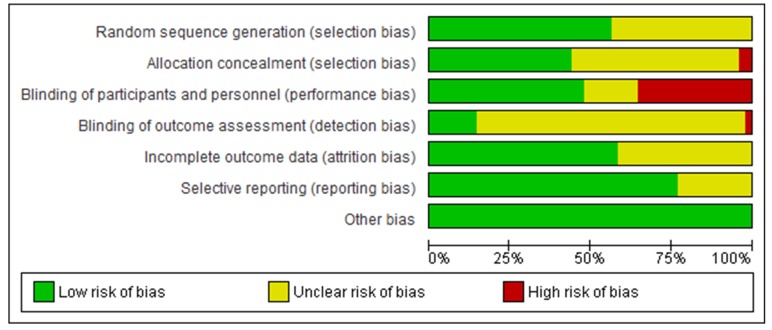
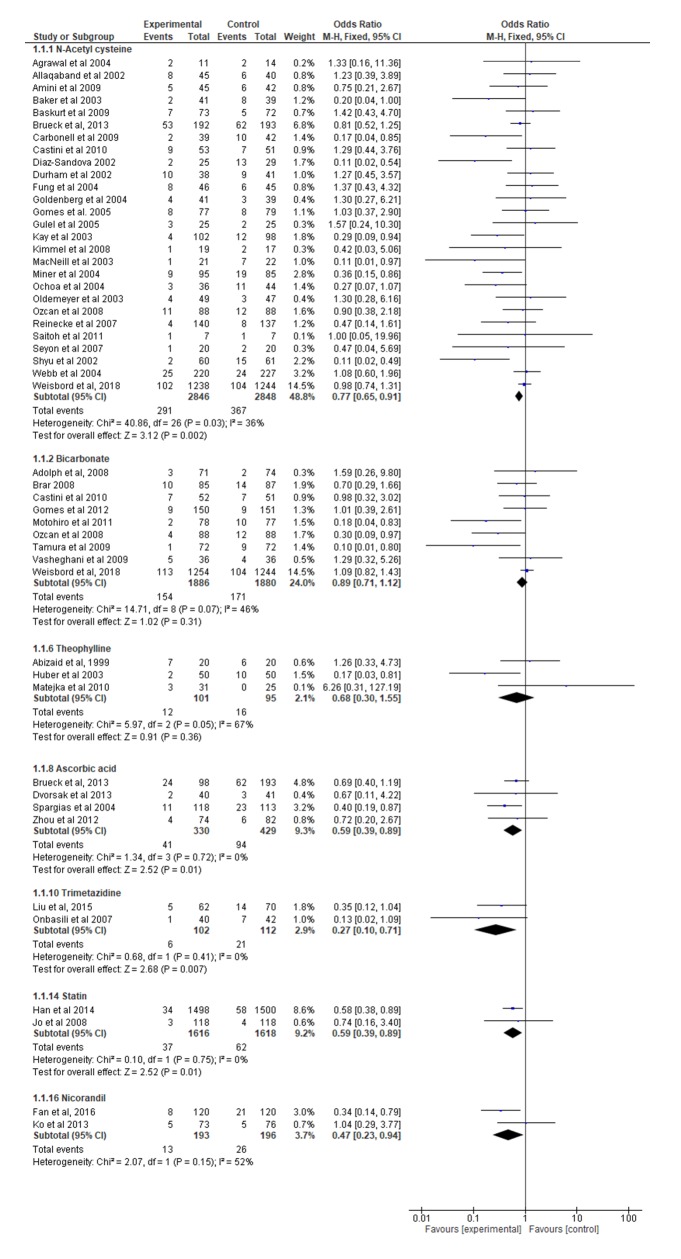
Results: Forty-eight RCTs were included. Seven pharmacological strategies were evaluated by multiple RCTs and 10 by one RCT each. These had varying risk of bias; >25% of trials were at high risk of performance bias. Five strategies significantly reduced the odds of CI-AKI: N-acetylcysteine (NAC) (27 trials, 5694 participants; OR=0.77, 95% CI 0.65 to 0.91, p=0.002, I2=36%), ascorbic acid (four trials, 759 participants; OR=0.59, 95% CI 0.39 to 0.89, p=0.01, I2=0%), statin (two trials, 3234 participants; OR=0.59, 95% CI 0.39 to 0.89, p=0.75, I2=0%), trimetazidine (two trials, 214 participants; OR=0.27, 95% CI 0.10 to 0.71, p=0.01, I2=0%) and nicorandil (two trials, 389 participants; OR=0.47, 95% CI 0.23 to 0.94, p=0.03, I2=52%). Theophylline had a similar, but non-significant, effect. A subgroup analysis found that the benefit of NAC was highest in patients requiring a high-contrast dose.
Conclusions: Several drugs are renoprotective in patients with CKD undergoing CAG±PCI. The evidence is strongest for NAC. We recommend that NAC should be used when a high dose of contrast is anticipated.
Trial registration number: PROSPERO registration CRD42014014704.Open Science Framework link: https://osf.io/vxg7d/?view_only=62bad0404b18405abd39ff2ead2575a8.
Keywords: Coronary angiography; contrast media; coronary intervention (PCI); renal disease.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Crimi G, Leonardi S, Costa F, et al. . Incidence, prognostic impact, and optimal definition of contrast-induced acute kidney injury in consecutive patients with stable or unstable coronary artery disease undergoing percutaneous coronary intervention. insights from the all-comer PRODIGY trial. Catheter Cardiovasc Interv 2015;86:E19–E27. 10.1002/ccd.25822 - DOI - PubMed
-
- KDIGOKAKIW KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int 2012;(Suppl 2):1–138.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous