

Turning the corner on therapeutic cancer vaccines
- PMID: 30774998
- PMCID: PMC6368616
- DOI: 10.1038/s41541-019-0103-y
Turning the corner on therapeutic cancer vaccines
Abstract
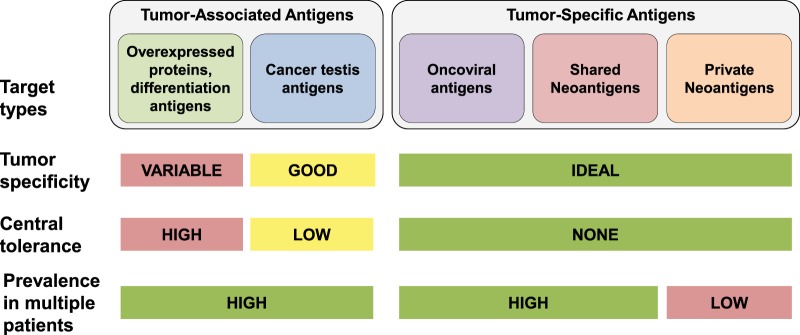
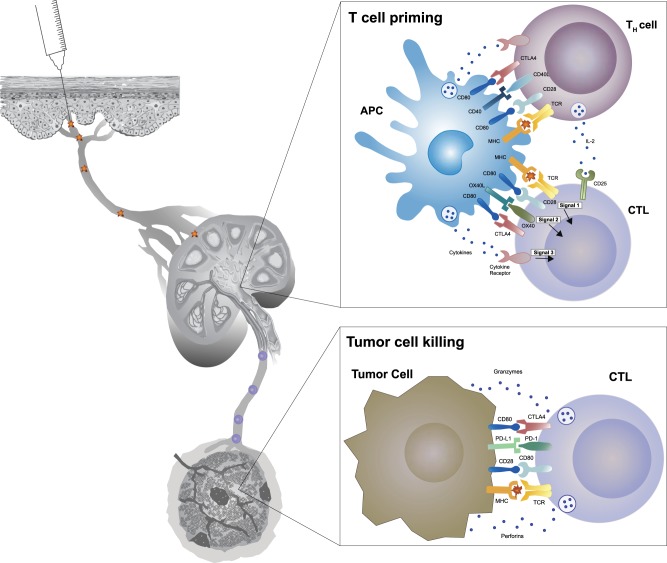
Recent advances in several areas are rekindling interest and enabling progress in the development of therapeutic cancer vaccines. These advances have been made in target selection, vaccine technology, and methods for reversing the immunosuppressive mechanisms exploited by cancers. Studies testing different tumor antigens have revealed target properties that yield high tumor versus normal cell specificity and adequate immunogenicity to affect clinical efficacy. A few tumor-associated antigens, normal host proteins that are abnormally expressed in cancer cells, have been demonstrated to serve as good targets for immunotherapies, although many do not possess the needed specificity or immunogenicity. Neoantigens, which arise from mutated proteins in cancer cells, are truly cancer-specific and can be highly immunogenic, though the vast majority are unique to each patient's cancer and thus require development of personalized therapies. Lessons from previous cancer vaccine expeditions are teaching us the type and magnitude of immune responses needed, as well as vaccine technologies that can achieve these responses. For example, we are learning which vaccine approaches elicit the potent, balanced, and durable CD4 plus CD8 T cell expansion necessary for clinical efficacy. Exploration of interactions between the immune system and cancer has elucidated the adaptations that enable cancer cells to suppress and evade immune attack. This has led to breakthroughs in the development of new drugs, and, subsequently, to opportunities to combine these with cancer vaccines and dramatically increase patient responses. Here we review this recent progress, highlighting key steps that are bringing the promise of therapeutic cancer vaccines within reach.
Conflict of interest statement
R.E.H. and K.J. are employees and shareholders of Pfizer Inc.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
