

Intrachiasmatic craniopharyngioma: Assessment of visual outcome with optical coherence tomography after complete surgical removal
- PMID: 30775061
- PMCID: PMC6357539
- DOI: 10.4103/sni.sni_292_18
Intrachiasmatic craniopharyngioma: Assessment of visual outcome with optical coherence tomography after complete surgical removal
Abstract
Background: Optic chiasm invasion by a craniopharyngioma (CP) is exceptional. Surgical treatment of intrachiasmatic CPs associates a high risk of chiasm injury, which should be properly addressed before surgery.
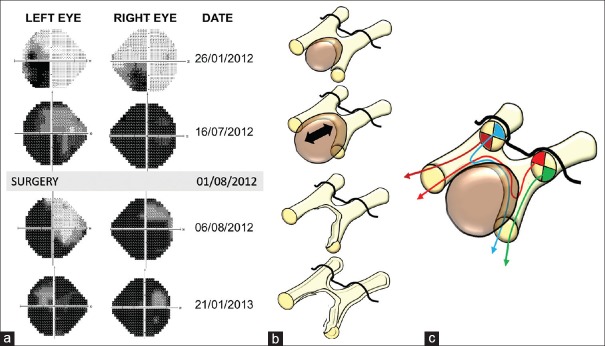
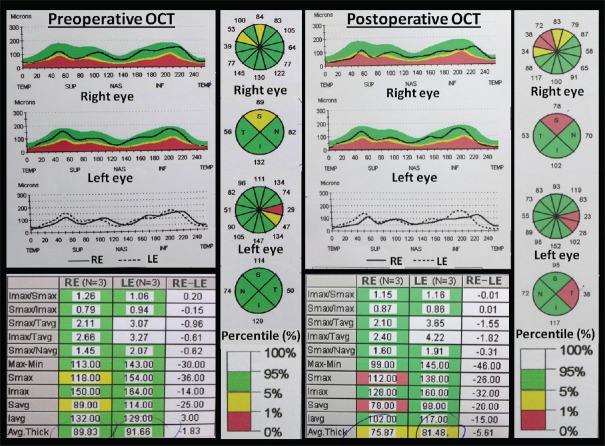
Case description: We present a 46-year-old woman admitted to the hospital with low visual acuity (0.1 in the right eye and 0.5 in the left) and a severe defect in her visual fields, in addition to headaches, diabetes insipidus, and a long-term depressive disorder. Her visual deficit progressed from a right homonymous temporal inferior quadrantanopia to an almost complete loss of vision in both eyes that only spared the upper nasal quadrants. Brain MRI showed a rounded third ventricle tumor with a potbelly expansion of the optic chiasm, suggesting chiasm invasion by the tumor. Optical coherence tomography (OCT) showed the thinning of the retinal nerve fiber layer (RNFL) in the superior and temporal wedges of the right eye and in the temporal wedge of the left one. The tumor was completely removed by employing a frontotemporal craniotomy and a translamina terminalis approach. Histological analysis showed a squamous-papillary CP. Postoperatively, a significant worsening of the visual defect was evidenced on the perimetry, which was related to a marked RNFL atrophy measured with OCT, as compared to the preoperative study. The poor long-term visual outcome in this patient correlated well with the results of postoperative OCT.
Conclusions: Preoperative analysis of retinal atrophy with optic coherence tomography allows a reliable assessment of the patient's visual outcome in CPs involving the optic chiasm.
Keywords: Craniopharyngioma; optic chiasm; optical coherence tomography; third ventricle; visual outcome.
Conflict of interest statement
There are no conflicts of interest
Figures



References
-
- Bialer OY, Goldenberg-Cohen N, Toledano H, Snir M, Michowiz S. Retinal NFL thinning on OCT correlates with visual field loss in pediatric craniopharyngioma. Can J Ophthalmol. 2013;48:494–9. - PubMed
-
- Brodsky MC, Hoyt WF, Barnwell SL, Wilson CB. Intrachiasmatic craniopharyngioma: A rare cause of chiasmal thickening. J Neurosurg. 1988;68:300–2. - PubMed
-
- Ciric IS, Cozzens JW. Craniopharyngiomas: Transsphenoidal method of approach -- for the virtuoso only? Clin Neurosurg. 1980;27:169–87. - PubMed
-
- Danesh-Meyer HV, Papchenko T, Savino PJ, Law A, Evans J, Gamble GD. In vivo retinal nerve fiber layer thickness measured by optical coherence tomography predicts visual recovery after surgery for parachiasmal tumors. Invest Ophthalmol Vis Sci. 2008;49:1879–85. - PubMed
-
- Duff TA, Levine R. Intrachiasmatic craniopharyngioma. Case Report. J Neurosurg. 1983;59:1766–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous