

Familial Melanoma: Diagnostic and Management Implications
- PMID: 30775140
- PMCID: PMC6368081
- DOI: 10.5826/dpc.0901a03
Familial Melanoma: Diagnostic and Management Implications
Abstract
Background: An estimated 5%-10% of all cutaneous melanoma cases occur in families. This review describes susceptibility genes currently known to be involved in melanoma predisposition, genetic testing of familial melanoma patients, and management implications.
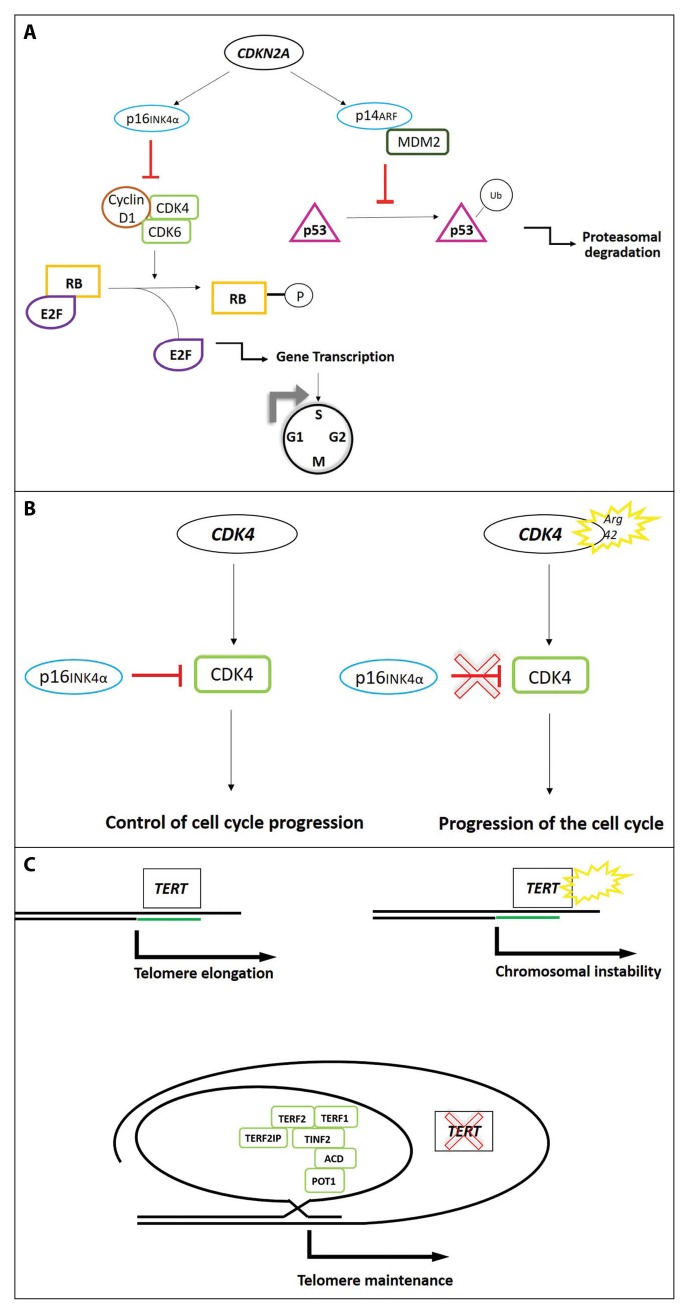
Results: CDKN2A is the major high-penetrance susceptibility gene with germline mutations identified in 20%-40% of melanoma families. A positive CDKN2A mutation status has been associated with a high number of affected family members, multiple primary melanomas, pancreatic cancer, and early age at melanoma onset. Mutations in the other melanoma predisposition genes-CDK4, BAP1, TERT, POT1, ACD, TERF2IP, and MITF-are rare, overall contributing to explain a further 10% of familial clustering of melanoma. The underlying genetic susceptibility remains indeed unexplained for half of melanoma families. Genetic testing for melanoma is currently recommended only for CDKN2A and CDK4, and, at this time, the role of multigene panel testing remains under debate. Individuals from melanoma families must receive genetic counseling to be informed about the inclusion criteria for genetic testing, the probability of an inconclusive result, the genetic risk for melanoma and other cancers, and the debatable role of medical management. They should be counseled focusing primarily on recommendations on appropriate lifestyle, encouraging skin self-examination, and regular dermatological screening.
Conclusions: Genetic testing for high-penetrance melanoma susceptibility genes is recommended in melanoma families after selection of the appropriate candidates and adequate counseling of the patient. All patients and relatives from melanoma kindreds, irrespective of their mutation status, should be encouraged to adhere to a correct ultraviolet exposure, skin self-examination, and surveillance by physicians.
Keywords: CDK4; CDKN2A; cancer screening; familial melanoma; genetic counseling; genetic testing.
Conflict of interest statement
Competing interests: The authors have no conflicts of interest to disclose.
Figures
References
-
- Nikolaou V, Stratigos AJ. Emerging trends in the epidemiology of melanoma. Br J Dermatol. 2014;170(1):11–19. - PubMed
-
- Balch CM, Buzaid AC, Soong SJ, et al. Final version of the American Joint Committee on Cancer staging system for cutaneous melanoma. J Clin Oncol. 2001;19(16):3635–3648. - PubMed
-
- Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma, I: common and atypical naevi. Eur J Cancer. 2005;41(1):28–44. - PubMed
-
- Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma, II: sun exposure. Eur J Cancer. 2005;41(1):45–60. - PubMed
-
- Gandini S, Sera F, Cattaruzza MS, et al. Meta-analysis of risk factors for cutaneous melanoma, III: family history, actinic damage and phenotypic factors. Eur J Cancer. 2005;41(14):2040–2059. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous