

Metastatic prostate cancer remains incurable, why?
- PMID: 30775246
- PMCID: PMC6363601
- DOI: 10.1016/j.ajur.2018.11.005
Metastatic prostate cancer remains incurable, why?
Abstract
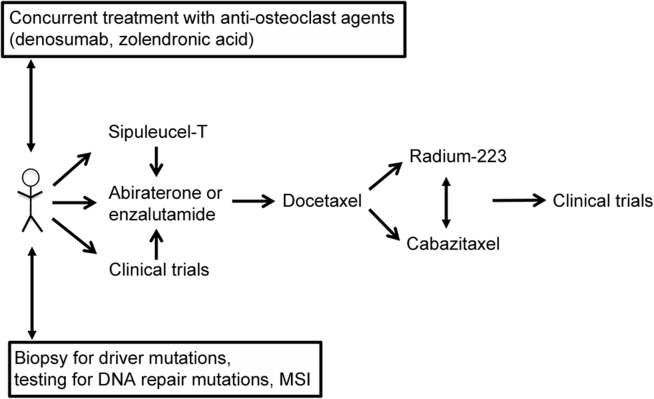
Metastatic prostate cancer patients present in two ways-with already disseminated disease at the time of presentation or with disease recurrence after definitive local therapy. Androgen deprivation therapy is given as the most effective initial treatment to patients. However, after the initial response, almost all patients will eventually progress despite the low levels of testosterone. Disease at this stage is termed castration resistant prostate cancer (CRPC). Before 2010, the taxane docetaxel was the first and only life prolonging agent for metastatic CRPC (mCRPC). The last decade has witnessed robust progress in CRPC therapeutics development. Abiraterone, enzalutamide, apalutamide and sipuleucel-T have been evaluated as first- and second-line agents in mCRPC patients, while cabazitaxel was approved as a second-line treatment. Radium-223 dichloride was approved in symptomatic patients with bone metastases and no known visceral metastases pre- and post-docetaxel. However, despite significant advances, mCRPC remains a lethal disease. Both primary and acquired resistance have been observed in CRPC patients treated by these new agents. It could be solely cell intrinsic or it is possible that the clonal heterogeneity in treated tumors may result from the adaptive responses to the selective pressures within the tumor microenvironment. The aim of this review is to list current treatment agents of CRPC and summarize recent findings in therapeutic resistance mechanisms.
Keywords: Drug resistance; Heterogeneity; Novel treatment; Prostate cancer.
Figures
References
-
- Arnold M., Karim-Kos H.E., Coebergh J.W., Byrnes G., Antilla A., Ferlay J. Recent trends in incidence of five common cancers in 26 European countries since 1988: analysis of the European cancer observatory. Eur J Cancer. 2015;51:1164–1187. - PubMed
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. - PubMed
-
- Ferlay J., Soerjomataram I., Dikshit R., Eser S., Mathers C., Rebelo M. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Bray F., Kiemeney L.A. Epidemiology of prostate cancer in Europe: patterns, trends and determinants. In: Bolla M., van Poppel H., editors. Management of prostate cancer: a multidisciplinary approach. Springer International Publishing; Cham: 2017. pp. 1–27.
-
- Chen W., Zheng R., Baade P.D., Zhang S., Zeng H., Bray F. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–132. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
