

Malignant ameloblastoma: a challenging diagnosis
- PMID: 30775320
- PMCID: PMC6360822
- DOI: 10.4322/acr.2018.043
Malignant ameloblastoma: a challenging diagnosis
Abstract
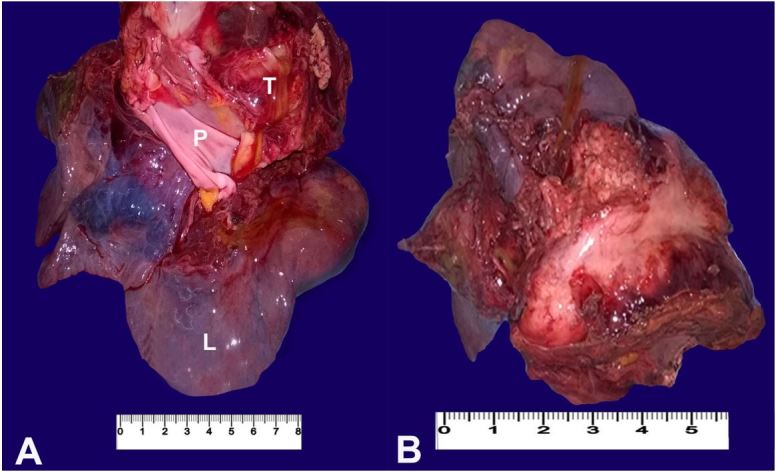
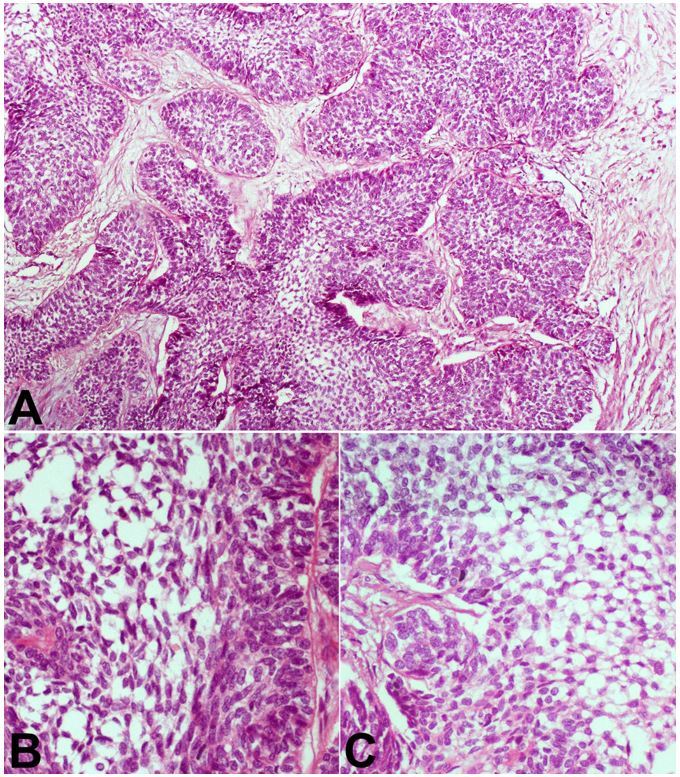
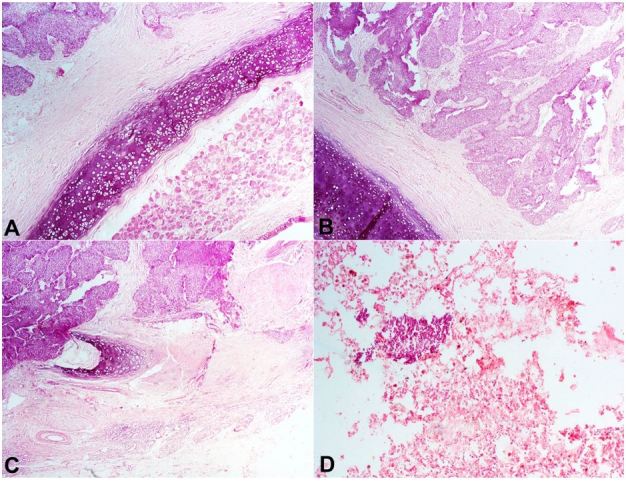
Ameloblastoma is an uncommon and locally aggressive, benign, odontogenic tumor, with local recurrence when not adequately excised. A rare variant of this neoplasm with the benign features but accompanied with metastases has been described. This rare variant is malignant ameloblastoma and is known to have a poor prognosis. We present the case of a young woman who had recurrent mandibular tumors, which were resected twice and histologically reported as ameloblastoma. Four years later, she presented with pulmonary metastasis and atelectasis. A review of the literature on this very rare neoplasm was also performed.
Keywords: Ameloblastoma; Mediastinum; Neoplasm Metastasis; Pulmonary Atelectasis.
Figures
References
-
- Ladeinde AL, Ogunlewe MO, Bamgbose BO, et al. . Ameloblastoma: analysis of 207 cases in a Nigerian teaching hospital. Quintessence Int. 2006;37(1):69-74. - PubMed
