

Human consciousness is supported by dynamic complex patterns of brain signal coordination
- PMID: 30775433
- PMCID: PMC6365115
- DOI: 10.1126/sciadv.aat7603
Human consciousness is supported by dynamic complex patterns of brain signal coordination
Abstract
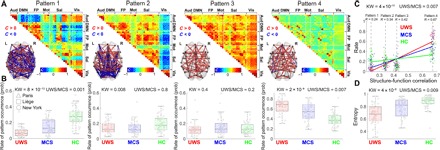
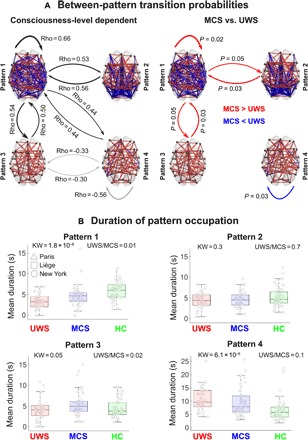
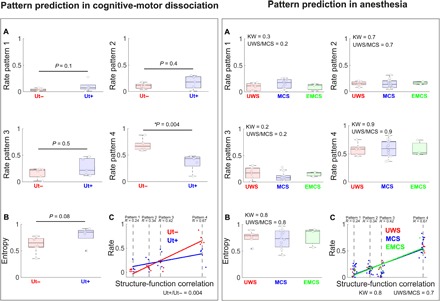
Adopting the framework of brain dynamics as a cornerstone of human consciousness, we determined whether dynamic signal coordination provides specific and generalizable patterns pertaining to conscious and unconscious states after brain damage. A dynamic pattern of coordinated and anticoordinated functional magnetic resonance imaging signals characterized healthy individuals and minimally conscious patients. The brains of unresponsive patients showed primarily a pattern of low interareal phase coherence mainly mediated by structural connectivity, and had smaller chances to transition between patterns. The complex pattern was further corroborated in patients with covert cognition, who could perform neuroimaging mental imagery tasks, validating this pattern's implication in consciousness. Anesthesia increased the probability of the less complex pattern to equal levels, validating its implication in unconsciousness. Our results establish that consciousness rests on the brain's ability to sustain rich brain dynamics and pave the way for determining specific and generalizable fingerprints of conscious and unconscious states.
Figures
References
-
- Stern P., Neuroscience: In search of new concepts. Science 358, 464–465 (2017). - PubMed
-
- Tononi G., Consciousness as integrated information: A provisional manifesto. Biol. Bull. 215, 216–242 (2008). - PubMed
-
- Northoff G., Huang Z., How do the brain’s time and space mediate consciousness and its different dimensions? Temporo-spatial theory of consciousness (TTC). Neurosci. Biobehav. Rev. 80, 630–645 (2017). - PubMed
-
- Dehaene S., Changeux J.-P., Experimental and theoretical approaches to conscious processing. Neuron 70, 200–227 (2011). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
