Assessing Spinal Cerebrospinal Fluid Leaks in Spontaneous Intracranial Hypotension With a Scoring System Based on Brain Magnetic Resonance Imaging Findings
- PMID: 30776059
- PMCID: PMC6515981
- DOI: 10.1001/jamaneurol.2018.4921
Assessing Spinal Cerebrospinal Fluid Leaks in Spontaneous Intracranial Hypotension With a Scoring System Based on Brain Magnetic Resonance Imaging Findings
Abstract
Importance: Various signs may be observed on brain magnetic resonance imaging (MRI) in patients with spontaneous intracranial hypotension (SIH). However, the lack of a classification system integrating these findings limits decision making in clinical practice.
Objective: To develop a probability score based on the most relevant brain MRI findings to assess the likelihood of an underlying spinal cerebrospinal fluid (CSF) leak in patients with SIH.
Design, setting, and participants: This case-control study in consecutive patients investigated for SIH was conducted at a single hospital department from February 2013 to October 2017. Patients with missing brain MRI data were excluded. Three blinded readers retrospectively reviewed the brain MRI scans of patients with SIH and a spinal CSF leak, patients with orthostatic headache without a CSF leak, and healthy control participants, evaluating 9 quantitative and 7 qualitative signs. A predictive diagnostic score based on multivariable backward logistic regression analysis was then derived. Its performance was validated internally in a prospective cohort of patients who had clinical suspicion for SIH.
Main outcomes and measures: Likelihood of a spinal CSF leak based on the proposed diagnostic score.
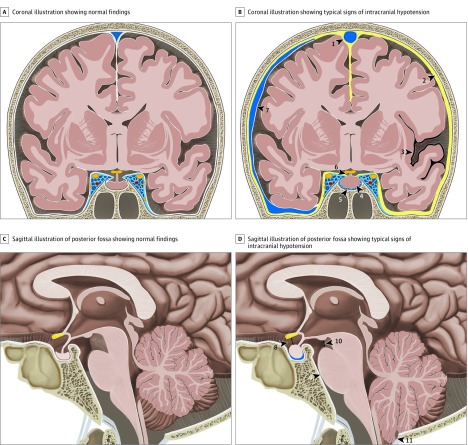
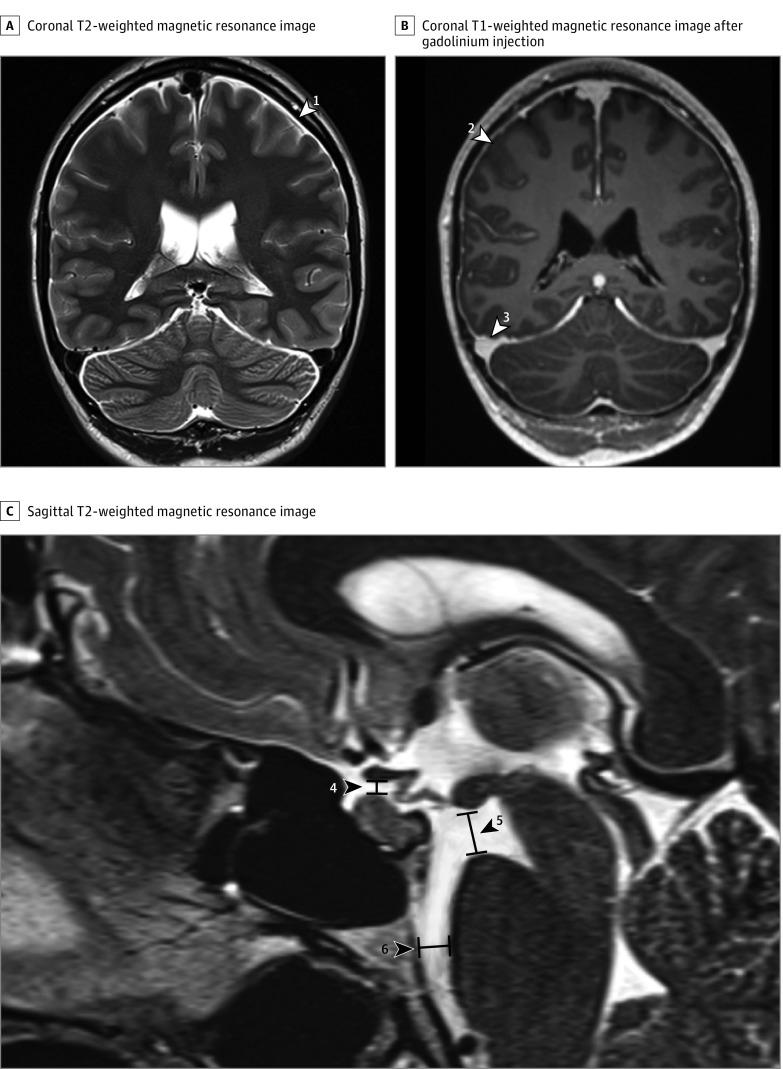
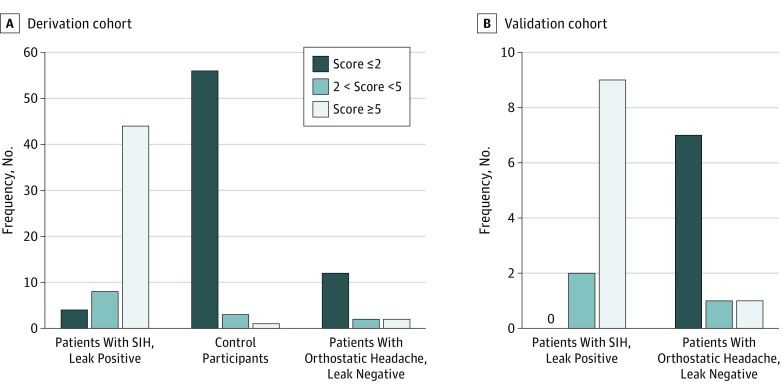
Results: A total of 152 participants (101 female [66.4%]; mean [SD] age, 46.1 [14.3] years) were studied. These included 56 with SIH and a spinal CSF leak, 16 with orthostatic headache without a CSF leak, 60 control participants, and 20 patients in the validation cohort. Six imaging findings were included in the final scoring system. Three were weighted as major (2 points each): pachymeningeal enhancement, engorgement of venous sinus, and effacement of the suprasellar cistern of 4.0 mm or less. Three were considered minor (1 point each): subdural fluid collection, effacement of the prepontine cistern of 5.0 mm or less, and mamillopontine distance of 6.5 mm or less. Patients were classified into groups at low, intermediate, or high probability of having a spinal CSF leak, with total scores of 2 points or fewer, 3 to 4 points, and 5 points or more, respectively, on a scale of 9 points. The discriminatory ability of the proposed score could be demonstrated in the validation cohort.
Conclusions and relevance: This 3-tier predictive scoring system is based on the 6 most relevant brain MRI findings and allows assessment of the likelihood (low, intermediate, or high) of a positive spinal imaging result in patients with SIH. It may be useful in identifying patients with SIH who are leak positive and in whom further invasive myelographic examinations are warranted before considering targeted therapy.
Conflict of interest statement
Figures