

Reduction of intrapancreatic neural density in cancer tissue predicts poorer outcome in pancreatic ductal carcinoma
- PMID: 30776178
- PMCID: PMC6447831
- DOI: 10.1111/cas.13975
Reduction of intrapancreatic neural density in cancer tissue predicts poorer outcome in pancreatic ductal carcinoma
Abstract
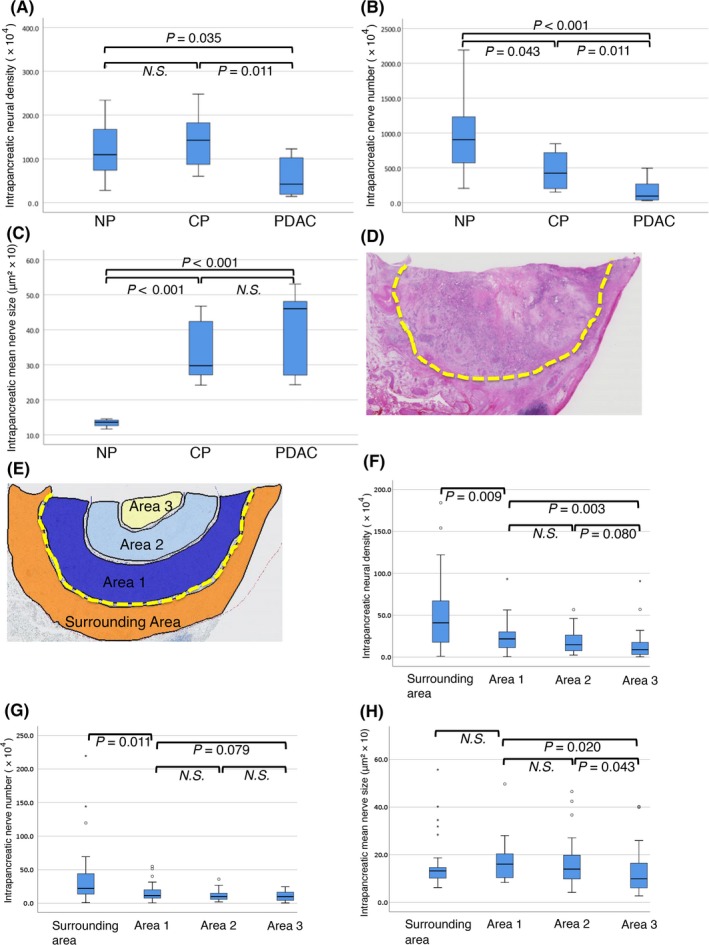
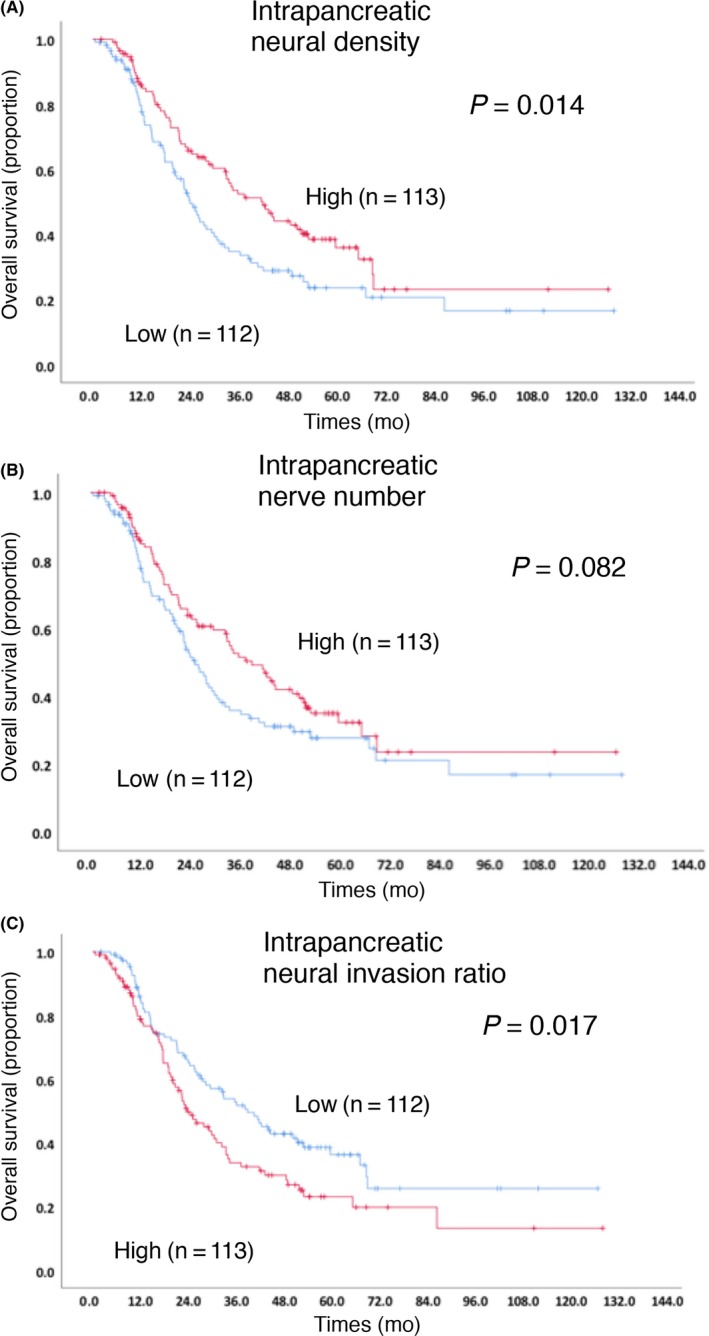
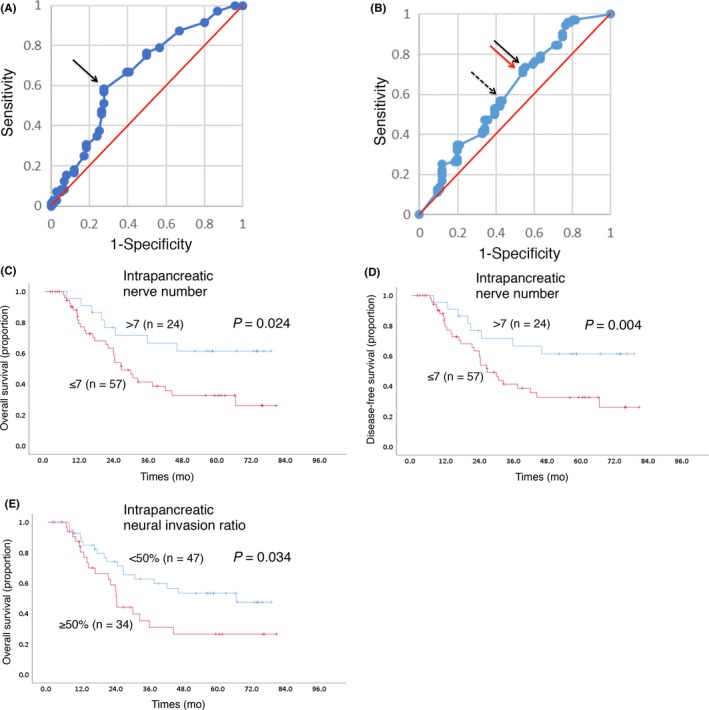
Neural invasion is one of the malignant features contributing to locally advanced and/or metastatic disease progression in patients with pancreatic ductal adenocarcinoma (PDAC). Few studies exist on the distribution and state of nerve fibers in PDAC tissue and their clinicopathological impacts. The aim of the present study was to investigate the clinicopathological characteristics and prognostic value of intrapancreatic neural alterations in patients with PDAC. We retrospectively analyzed 256 patients with PDAC who underwent macroscopic curative surgery. Nerve fibers, immunolabeled with a specific neural marker GAP-43, were digitally counted and compared among PDAC, chronic pancreatitis (CP) and normal pancreatic tissues. Interlobular nerve fibers were apparently hypertrophic in both CP and PDAC, although intrapancreatic neural density and nerve number decreased characteristically in PDAC. They tended to decrease toward the center of the tumor. Kaplan-Meier survival analyses revealed a statistically significant correlation between low neural density and shorter overall survival (OS) (P = 0.014), and between high neural invasion and shorter OS (P = 0.017). Neural density (P = 0.04; HR = 1.496; 95% CI 1.018-2.199) and neural invasion ratio (P = 0.064; HR = 1.439; 95% CI .980-2.114) were prognostic factors of shorter OS in the multivariate analysis. These findings suggest low intrapancreatic neural density in patients with PDAC as an independent prognosticator, which may represent aggressive tumor behavior. Furthermore, we propose a simple, practical and reproducible method (to measure neural density and the neural invasion ratio during conventional histopathological diagnosis of PDAC), which has been validated using another cohort (n = 81).
Keywords: ductal carcinoma; intrapancreatic neural density; intrapancreatic neural invasion; pancreas; prognosis.
© 2019 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Figures

Similar articles
-
Clinicopathological correlations of nestin expression in surgically resectable pancreatic cancer including an analysis of perineural invasion.J Gastrointestin Liver Dis. 2011 Dec;20(4):389-96. J Gastrointestin Liver Dis. 2011. PMID: 22187705
-
Intrapancreatic nerve invasion as a predictor for recurrence after pancreaticoduodenectomy in patients with invasive ductal carcinoma of the pancreas.Pancreas. 2011 Apr;40(3):464-8. doi: 10.1097/MPA.0b013e31820b5d37. Pancreas. 2011. PMID: 21289526
-
Linc00675 is a novel marker of short survival and recurrence in patients with pancreatic ductal adenocarcinoma.World J Gastroenterol. 2015 Aug 21;21(31):9348-57. doi: 10.3748/wjg.v21.i31.9348. World J Gastroenterol. 2015. PMID: 26309360 Free PMC article.
-
Different clinical presentations of metachronous pulmonary metastases after resection of pancreatic ductal adenocarcinoma: Retrospective study and review of the literature.World J Gastroenterol. 2017 Sep 21;23(35):6420-6428. doi: 10.3748/wjg.v23.i35.6420. World J Gastroenterol. 2017. PMID: 29085191 Free PMC article. Review.
-
The clinicopathological and prognostic significance of PD-L1 expression in pancreatic cancer: A meta-analysis.Hepatobiliary Pancreat Dis Int. 2018 Apr;17(2):95-100. doi: 10.1016/j.hbpd.2018.03.007. Epub 2018 Mar 13. Hepatobiliary Pancreat Dis Int. 2018. PMID: 29576277 Review.
Cited by
-
Pancreatic Ductal Adenocarcinoma Induces Neural Injury that Promotes a Transcriptomic and Functional Repair Signature by Peripheral Neuroglia.Res Sq [Preprint]. 2023 Mar 28:rs.3.rs-2715023. doi: 10.21203/rs.3.rs-2715023/v1. Res Sq. 2023. Update in: Oncogene. 2023 Aug;42(34):2536-2546. doi: 10.1038/s41388-023-02775-7. PMID: 37034696 Free PMC article. Updated. Preprint.
-
Pancreatic ductal adenocarcinoma induces neural injury that promotes a transcriptomic and functional repair signature by peripheral neuroglia.Oncogene. 2023 Aug;42(34):2536-2546. doi: 10.1038/s41388-023-02775-7. Epub 2023 Jul 11. Oncogene. 2023. PMID: 37433986 Free PMC article.
-
Targeting the peripheral neural-tumour microenvironment for cancer therapy.Nat Rev Drug Discov. 2024 Oct;23(10):780-796. doi: 10.1038/s41573-024-01017-z. Epub 2024 Sep 6. Nat Rev Drug Discov. 2024. PMID: 39242781 Free PMC article. Review.
-
The supporting role of Schwann cells in perineural invasion of pancreatic ductal adenocarcinoma.Front Pharmacol. 2025 Jun 11;16:1540027. doi: 10.3389/fphar.2025.1540027. eCollection 2025. Front Pharmacol. 2025. PMID: 40567365 Free PMC article. Review.
-
Investigation of Neural Microenvironment in Prostate Cancer in Context of Neural Density, Perineural Invasion, and Neuroendocrine Profile of Tumors.Front Oncol. 2021 Jul 1;11:710899. doi: 10.3389/fonc.2021.710899. eCollection 2021. Front Oncol. 2021. PMID: 34277455 Free PMC article.
References
-
- Hidalgo M. Pancreatic cancer. N Engl J Med. 2010;362:1605‐1617. - PubMed
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913‐2921. - PubMed
-
- Greer JB, Brand RE. New developments in pancreatic cancer. Curr Gastroenterol Rep. 2011;13:131‐139. - PubMed
-
- Huguet F, Orthuon A, Touboul E, Marseguerra R, Mornex F. Pancreatic cancer. Cancer Radiother. 2010;14(Suppl 1):S94‐S102. - PubMed
-
- Chadha AS, Khoo A, Aliru ML, Arora HK, Gunther JR, Krishnan S. Recent advances and prospects for multimodality therapy in pancreatic cancer. Semin Radiat Oncol. 2016;26:320‐337. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
