

Effect of a Nurse-Led Preventive Psychological Intervention on Symptoms of Posttraumatic Stress Disorder Among Critically Ill Patients: A Randomized Clinical Trial
- PMID: 30776295
- PMCID: PMC6439605
- DOI: 10.1001/jama.2019.0073
Effect of a Nurse-Led Preventive Psychological Intervention on Symptoms of Posttraumatic Stress Disorder Among Critically Ill Patients: A Randomized Clinical Trial
Abstract
Importance: A meta-analysis of outcomes during the 6 months after intensive care unit (ICU) discharge indicate a prevalence for clinically important posttraumatic stress disorder (PTSD) symptoms of 25%.
Objective: To determine whether a nurse-led preventive, complex psychological intervention, initiated in the ICU, reduces patient-reported PTSD symptom severity at 6 months.
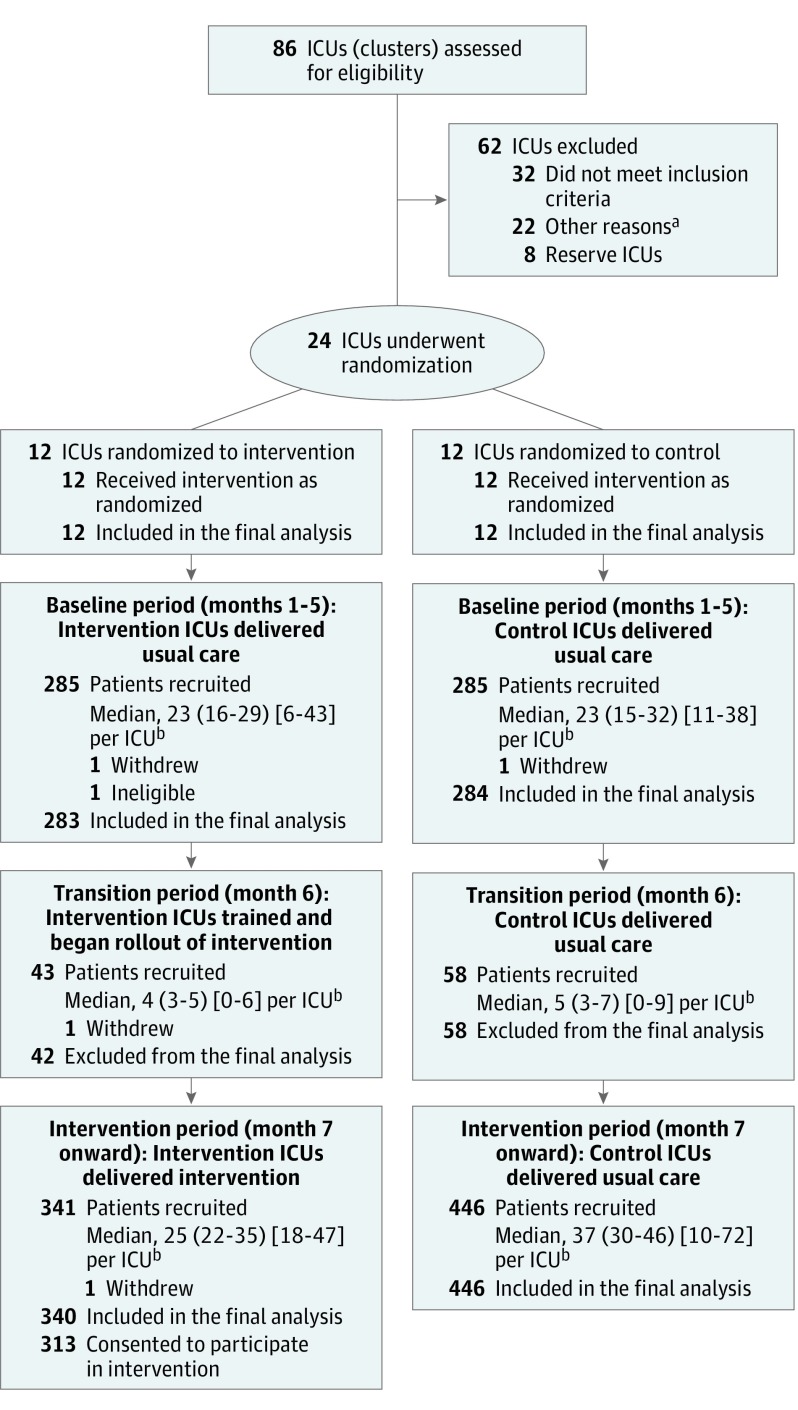
Design, setting, and participants: A multicenter, parallel-group, cluster-randomized clinical trial with integrated economic and process evaluations conducted in 24 ICUs in the United Kingdom. Participants were critically ill patients who regained mental capacity following receipt of level 3 (intensive) care. A total of 2961 eligible patients were identified from September 2015 to January 2017. A total of 2048 were approached for participation in the ICU, of which 1458 provided informed consent. Follow-up was completed December 2017.
Interventions: Twenty four ICUs were randomized 1:1 to the intervention or control group. Intervention ICUs (n = 12; 669 participants) delivered usual care during a baseline period followed by an intervention period. The preventive, complex psychological intervention comprised promotion of a therapeutic ICU environment plus 3 stress support sessions and a relaxation and recovery program delivered by trained ICU nurses to high-risk (acutely stressed) patients. Control ICUs (n = 12; 789 participants) delivered usual care in both baseline and intervention periods.
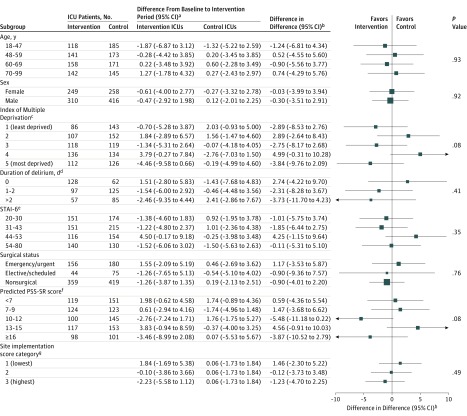
Main outcomes and measures: The primary clinical outcome was PTSD symptom severity among survivors at 6 months measured using the PTSD Symptom Scale-Self-Report questionnaire (score range, 0-51, with higher scores indicating greater symptom severity; the minimal clinically important difference was considered to be 4.2 points).
Results: Among 1458 enrolled patients (mean [SD] age, 58 [16] years; 599 women [41%]), 1353 (93%) completed the study and were included in the final analysis. At 6 months, the mean PTSD Symptom Scale-Self-Report questionnaire score in intervention ICUs was 11.8 (baseline period) compared with 11.5 (intervention period) (difference, -0.40 [95% CI, -2.46 to 1.67]) and in control ICUs, 10.1 (baseline period) compared with 10.2 (intervention period) (difference, 0.06 [95% CI, -1.74 to 1.85]) between periods. There was no significant difference in PTSD symptom severity at 6 months (treatment effect estimate [difference in differences] of -0.03 [95% CI, -2.58 to 2.52]; P = .98).
Conclusions and relevance: Among critically ill patients in the ICU, a nurse-led preventive, complex psychological intervention did not significantly reduce patient-reported PTSD symptom severity at 6 months. These findings do not support the use of this psychological intervention.
Trial registration: ISRCTN53448131.
Conflict of interest statement
Figures
Comment in
-
Addressing the Psychological Symptoms of Critical Illness: The Importance of "Negative" Trials in Guiding Next Steps.JAMA. 2019 Feb 19;321(7):649-650. doi: 10.1001/jama.2019.0072. JAMA. 2019. PMID: 30776299 No abstract available.
References
-
- Wade DF, Moon Z, Windgassen SS, Harrison AM, Morris L, Weinman JA. Non-pharmacological interventions to reduce ICU-related psychological distress: a systematic review. Minerva Anestesiol. 2016;82(4):465-478. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
