

HLA-A*32:01 is strongly associated with vancomycin-induced drug reaction with eosinophilia and systemic symptoms
- PMID: 30776417
- PMCID: PMC6612297
- DOI: 10.1016/j.jaci.2019.01.045
HLA-A*32:01 is strongly associated with vancomycin-induced drug reaction with eosinophilia and systemic symptoms
Abstract
Background: Vancomycin is a prevalent cause of the severe hypersensitivity syndrome drug reaction with eosinophilia and systemic symptoms (DRESS), which leads to significant morbidity and mortality and commonly occurs in the setting of combination antibiotic therapy, affecting future treatment choices. Variations in HLA class I in particular have been associated with serious T cell-mediated adverse drug reactions, which has led to preventive screening strategies for some drugs.
Objective: We sought to determine whether variation in the HLA region is associated with vancomycin-induced DRESS.
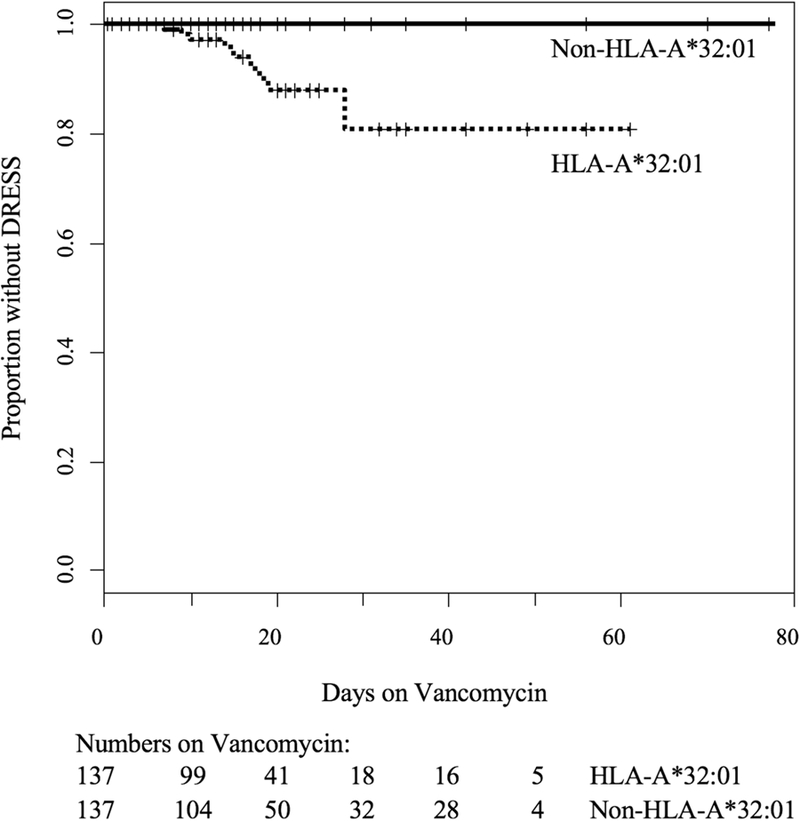
Methods: Probable vancomycin-induced DRESS cases were matched 1:2 with tolerant control subjects based on sex, race, and age by using BioVU, Vanderbilt's deidentified electronic health record database. Associations between DRESS and carriage of HLA class I and II alleles were assessed by means of conditional logistic regression. An extended sample set from BioVU was used to conduct a time-to-event analysis of those exposed to vancomycin with and without the identified HLA risk allele.
Results: Twenty-three subjects met the inclusion criteria for vancomycin-associated DRESS. Nineteen (82.6%) of 23 cases carried HLA-A*32:01 compared with 0 (0%) of 46 of the matched vancomycin-tolerant control subjects (P = 1 × 10-8) and 6.3% of the BioVU population (n = 54,249, P = 2 × 10-16). Time-to-event analysis of DRESS development during vancomycin treatment among the HLA-A*32:01-positive group indicated that 19.2% had DRESS and did so within 4 weeks.
Conclusions: HLA-A*32:01 is strongly associated with vancomycin-induced DRESS in a population of predominantly European ancestry. HLA-A*32:01 testing could improve antibiotic safety, help implicate vancomycin as the causal drug, and preserve future treatment options with coadministered antibiotics.
Keywords: T-cell hypersensitivity; Vancomycin; antibiotic allergy; delayed hypersensitivity; drug reaction with eosinophilia and systemic symptoms; human leukocyte antigen.
Copyright © 2019 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures



Comment in
-
HLA- and immune-mediated adverse drug reactions: Another hit with vancomycin.J Allergy Clin Immunol. 2019 Jul;144(1):44-45. doi: 10.1016/j.jaci.2019.04.009. Epub 2019 Apr 25. J Allergy Clin Immunol. 2019. PMID: 31029771 No abstract available.
References
-
- Lin YF, Yang CH, Sindy H, Lin JY, Rosaline Hui CY, Tsai YC, et al. Severe cutaneous adverse reactions related to systemic antibiotics. Clin Infect Dis 2014;58(10):1377–85. - PubMed
-
- Pavlos R, Mallal S, Phillips E. HLA and pharmacogenetics of drug hypersensitivity. Pharmacogenomics 2012;13(11):1285–306. - PubMed
-
- Aota N, Shiohara T. Viral connection between drug rashes and autoimmune diseases: how autoimmune responses are generated after resolution of drug rashes. Autoimmun Rev 2009;8(6):488–94. - PubMed
-
- Ghislain PD, Roujeau JC. Treatment of severe drug reactions: Stevens-Johnson syndrome, toxic epidermal necrolysis and hypersensitivity syndrome. Dermatol Online J 2002;8(1):5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AI110527/AI/NIAID NIH HHS/United States
- R01 AI134648/AI/NIAID NIH HHS/United States
- K12 HL143956/HL/NHLBI NIH HHS/United States
- T32 GM007347/GM/NIGMS NIH HHS/United States
- UL1 RR024975/RR/NCRR NIH HHS/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- R01 HD074711/HD/NICHD NIH HHS/United States
- R21 AI139021/AI/NIAID NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- R34 AI136815/AI/NIAID NIH HHS/United States
- T32 AI007474/AI/NIAID NIH HHS/United States
- U19 HL065962/HL/NHLBI NIH HHS/United States
- U01 HG006378/HG/NHGRI NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
- RC2 GM092618/GM/NIGMS NIH HHS/United States
- F30 AI131780/AI/NIAID NIH HHS/United States
- U01 HG004798/HG/NHGRI NIH HHS/United States
- P50 GM115305/GM/NIGMS NIH HHS/United States
- S10 RR025141/RR/NCRR NIH HHS/United States
- R01 NS032830/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
