

Fluid resuscitation with 0.9% saline alters haemostasis in an ovine model of endotoxemic shock
- PMID: 30776686
- PMCID: PMC7613520
- DOI: 10.1016/j.thromres.2019.02.015
Fluid resuscitation with 0.9% saline alters haemostasis in an ovine model of endotoxemic shock
Abstract
Introduction: Fluid resuscitation is a cornerstone of severe sepsis management, however there are many uncertainties surrounding the type and volume of fluid that is administered. The entire spectrum of coagulopathies can be seen in sepsis, from asymptomatic aberrations to fulminant disseminated intravascular coagulation (DIC). The aim of this study was to determine if fluid resuscitation with saline contributes to the haemostatic derangements in an ovine model of endotoxemic shock.
Materials and methods: Twenty-one adult female sheep were randomly divided into no endotoxemia (n = 5) or endotoxemia groups (n = 16) with an escalating dose of lipopolysaccharide (LPS) up to 4 μg/kg/h administered to achieve a mean arterial pressure below 60 mmHg. Endotoxemia sheep received either no bolus fluid resuscitation (n = 8) or a 0.9% saline bolus (40 mL/kg over 60 min) (n = 8). No endotoxemia, saline only animals (n = 5) underwent fluid resuscitation with a 0.9% bolus of saline as detailed above. Hemodynamic support with vasopressors was initiated if needed, to maintain a mean arterial pressure (MAP) of 60-65 mm Hg in all the groups.
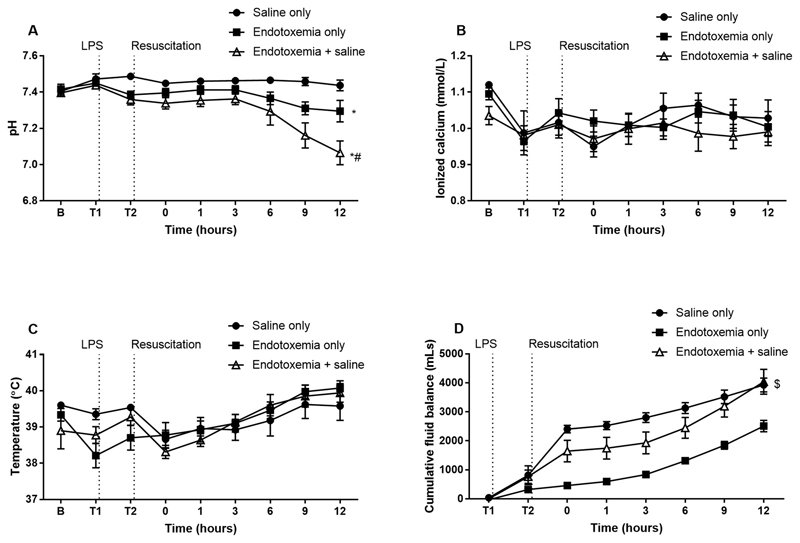
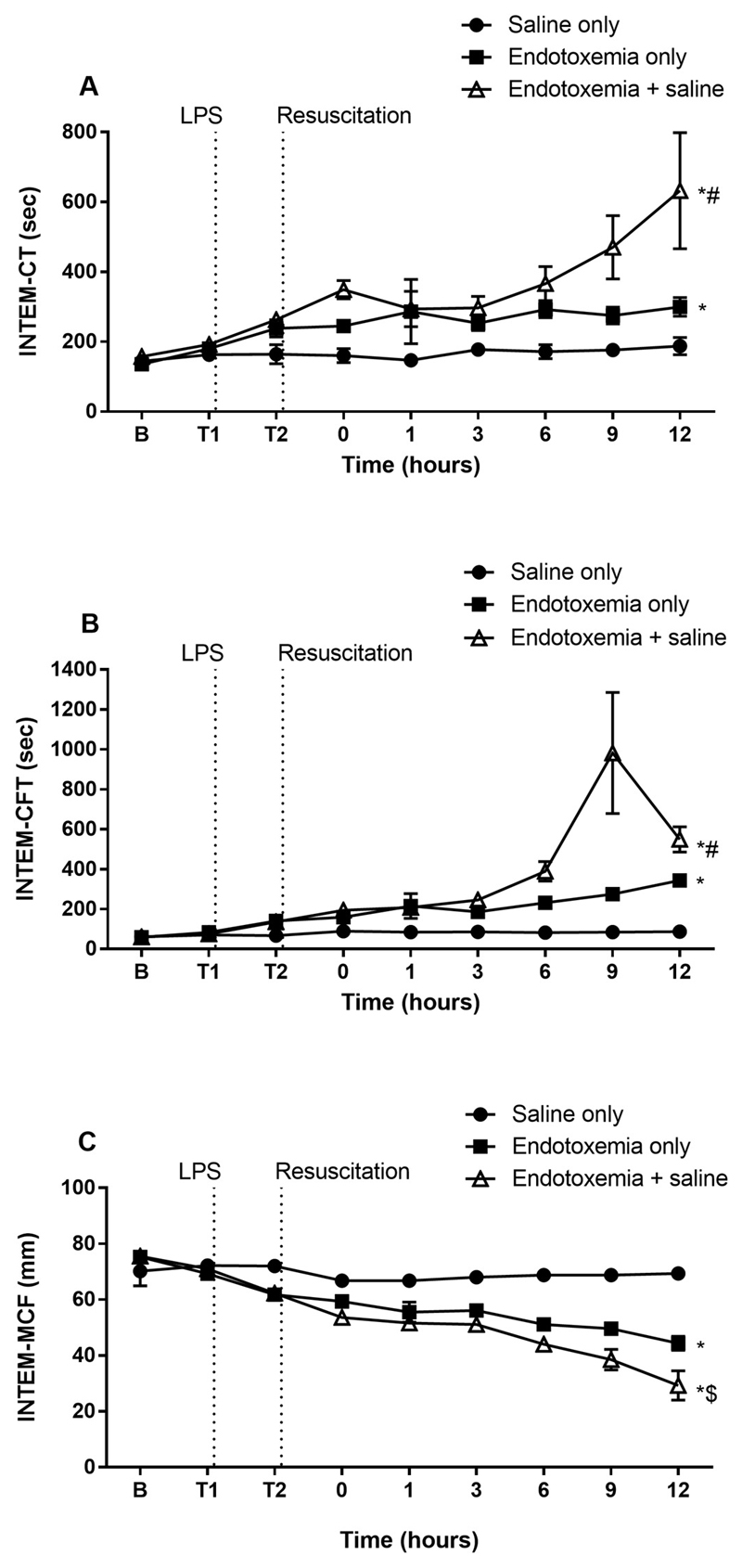
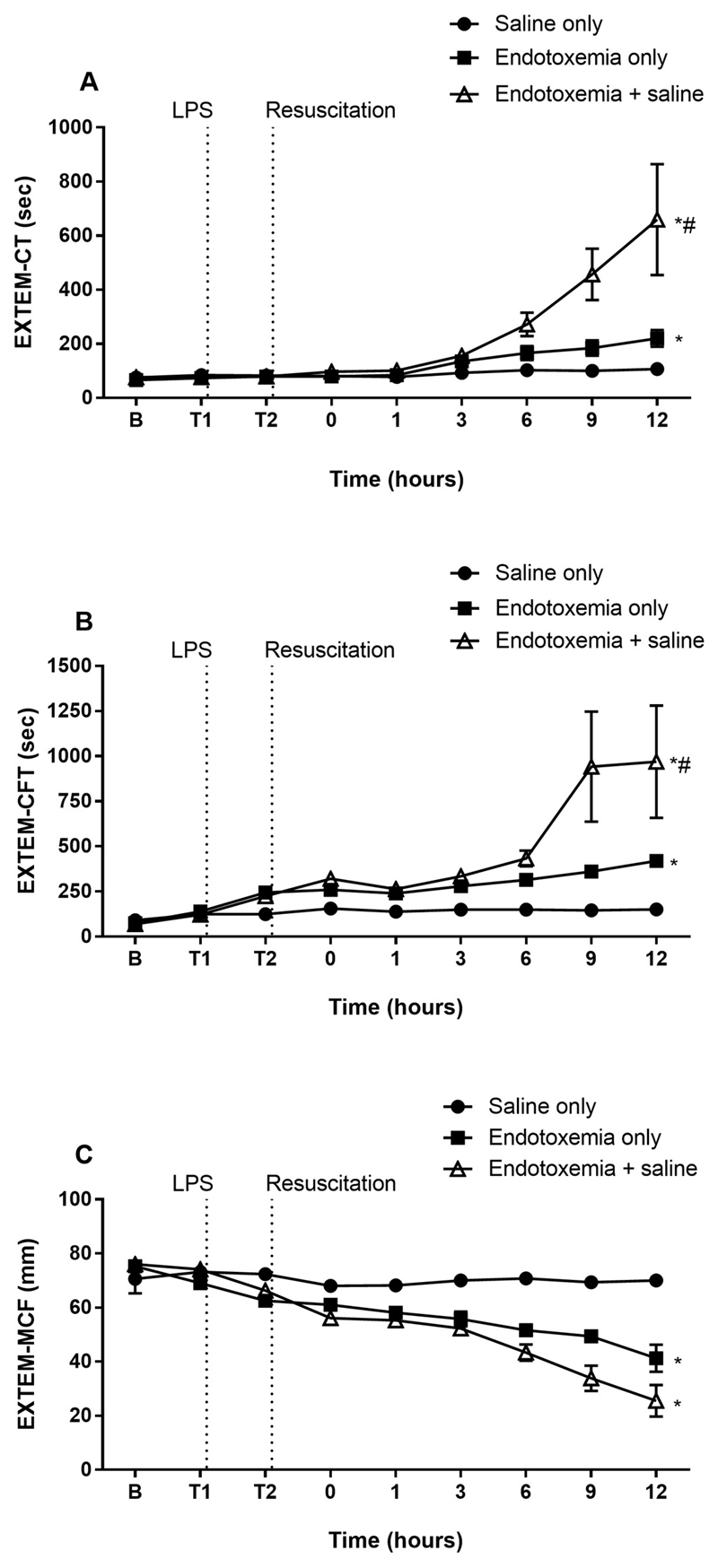
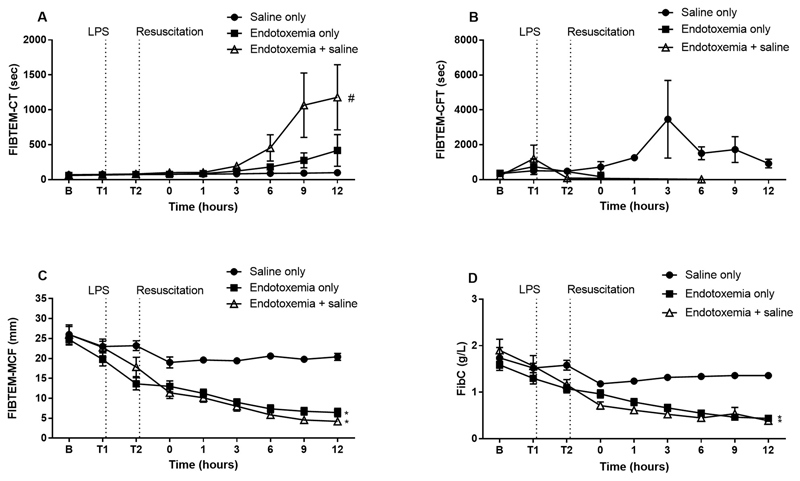
Results: Rotational thromboelastometry (ROTEM®) and conventional coagulation biomarker tests demonstrated sepsis induced derangements to secondary haemostasis. This effect was exacerbated by saline fluid resuscitation, with low pH (p = 0.036), delayed clot initiation and formation together with deficiencies in naturally occurring anti-coagulants antithrombin (p = 0.027) and Protein C (p = 0.001).
Conclusions: Endotoxemia impairs secondary haemostasis and induces changes in the intrinsic, extrinsic and anti-coagulant pathways. These changes to haemostasis are exacerbated following resuscitation with 0.9% saline, a commonly used crystalloid in clinical settings.
Keywords: Coagulation; Coagulation factors; Fibrinogen; Sepsis; Thromboelastometry.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
JFF received funding from the Office of Health and Medical Research, Queensland Health. The remaining authors declare no competing financial interests
Figures
References
-
- Vincent JL, Marshall JC, Namendys-Silva SA, Francois B, Martin-Loeches I, Lipman J, Reinhart K, Antonelli M, Pickkers P, Njimi H, Jimenez E, et al. Icon investigators, Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014;2:380–386. - PubMed
-
- Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, Jahan R, Harvey SE, Bell D, Bion JF, Coats TJ, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372:1301–1311. - PubMed
-
- Young P, Bailey M, Beasley R, Henderson S, Mackle D, McArthur C, McGuinness S, Mehrtens J, Myburgh J, Psirides A, Reddy S, et al. Effect of a Buffered Crystalloid Solution vs Saline on Acute Kidney Injury Among Patients in the Intensive Care Unit: The SPLIT Randomized Clinical Trial. JAMA. 2015;314:1701–1710. - PubMed
-
- Peake SL, Delaney A, Bailey M, Bellomo R, Cameron PA, Cooper DJ, Higgins AM, Holdgate A, Howe BD, Webb SA, Williams P. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371:1496–1506. - PubMed
