

Intravenous pulse methylprednisolone for induction of remission in severe ANCA associated Vasculitis: a multi-center retrospective cohort study
- PMID: 30777023
- PMCID: PMC6378728
- DOI: 10.1186/s12882-019-1226-0
Intravenous pulse methylprednisolone for induction of remission in severe ANCA associated Vasculitis: a multi-center retrospective cohort study
Abstract
Background: Intravenous pulse methylprednisolone (MP) is commonly included in the management of severe ANCA associated vasculitis (AAV) despite limited evidence of benefit. We aimed to evaluate outcomes in patients who had, or had not received MP, along with standard therapy for remission induction in severe AAV.
Methods: We retrospectively studied 114 consecutive patients from five centres in Europe and the United States with a new diagnosis of severe AAV (creatinine > 500 μmol/L or dialysis dependency) and that received standard therapy (plasma exchange, cyclophosphamide and high-dose oral corticosteroids) for remission induction with or without pulse MP between 2000 and 2013. We evaluated survival, renal recovery, relapses, and adverse events over the first 12 months.
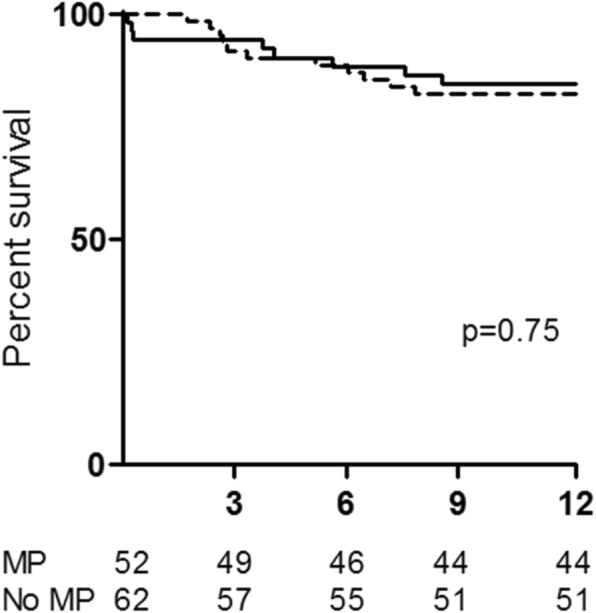
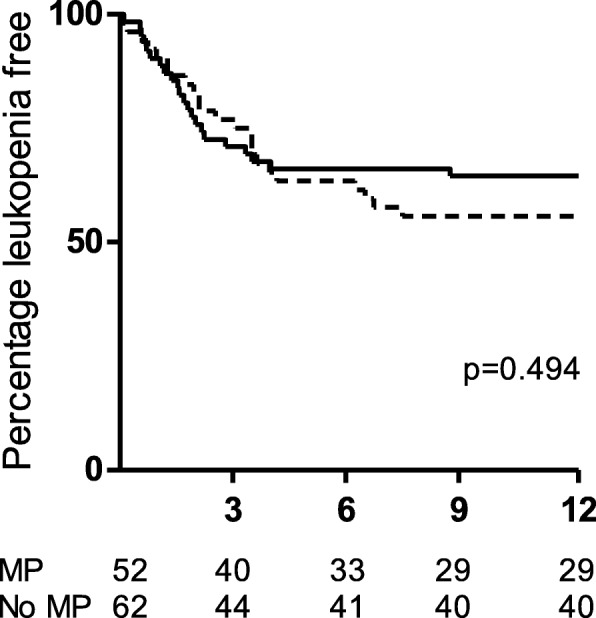
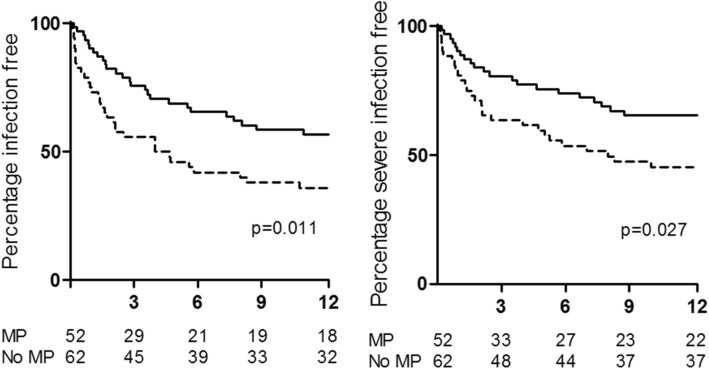
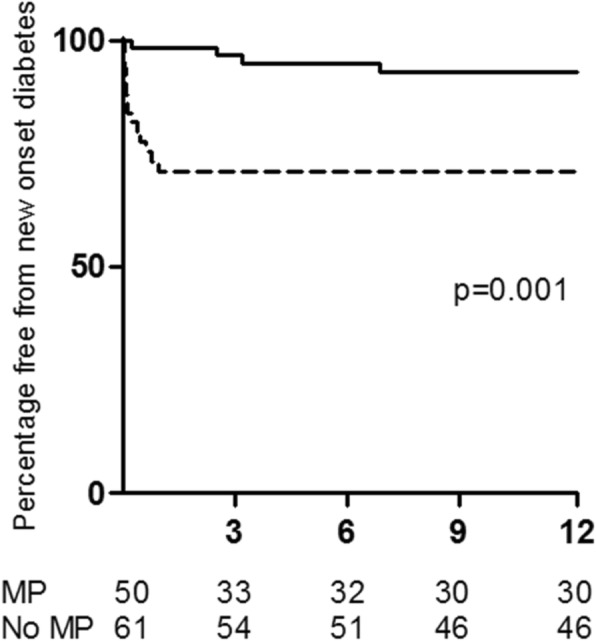
Results: Fifty-two patients received pulse MP in addition to standard therapy compared to 62 patients that did not. There was no difference in survival, renal recovery or relapses. Treatment with MP associated with higher risk of infection during the first 3 months (hazard ratio (HR) 2.7, 95%CI [1.4-5.3], p = 0.004) and higher incidence of diabetes (HR 6.33 [1.94-20.63], p = 0.002), after adjustment for confounding factors.
Conclusions: The results of this study suggest that addition of pulse intravenous MP to standard therapy for remission induction in severe AAV may not confer clinical benefit and may be associated with more episodes of infection and higher incidence of diabetes.
Keywords: ANCA; Diabetes mellitus; Infection; Methylprednisolone; Vasculitis.
Conflict of interest statement
Ethics approval and cosent to participate
This was a quality improvement project where data was collected as part of routine clinical care. Furthermore patients were diagnosed and treated according to currently accepted recommendations. The purpose of this analysis was improvement of clinical care rather than primary research. The authors had access to the data as part of their role as care providers to the patients involved however all data was anonymised at the data collection stage. For these reasons ethical approval and / or patient consent was not sought. This was discussed and agreed with the R&D Department at University Hospital Birmingham.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
