

Targeting DNA Damage Response Promotes Antitumor Immunity through STING-Mediated T-cell Activation in Small Cell Lung Cancer
- PMID: 30777870
- PMCID: PMC6563834
- DOI: 10.1158/2159-8290.CD-18-1020
Targeting DNA Damage Response Promotes Antitumor Immunity through STING-Mediated T-cell Activation in Small Cell Lung Cancer
Abstract
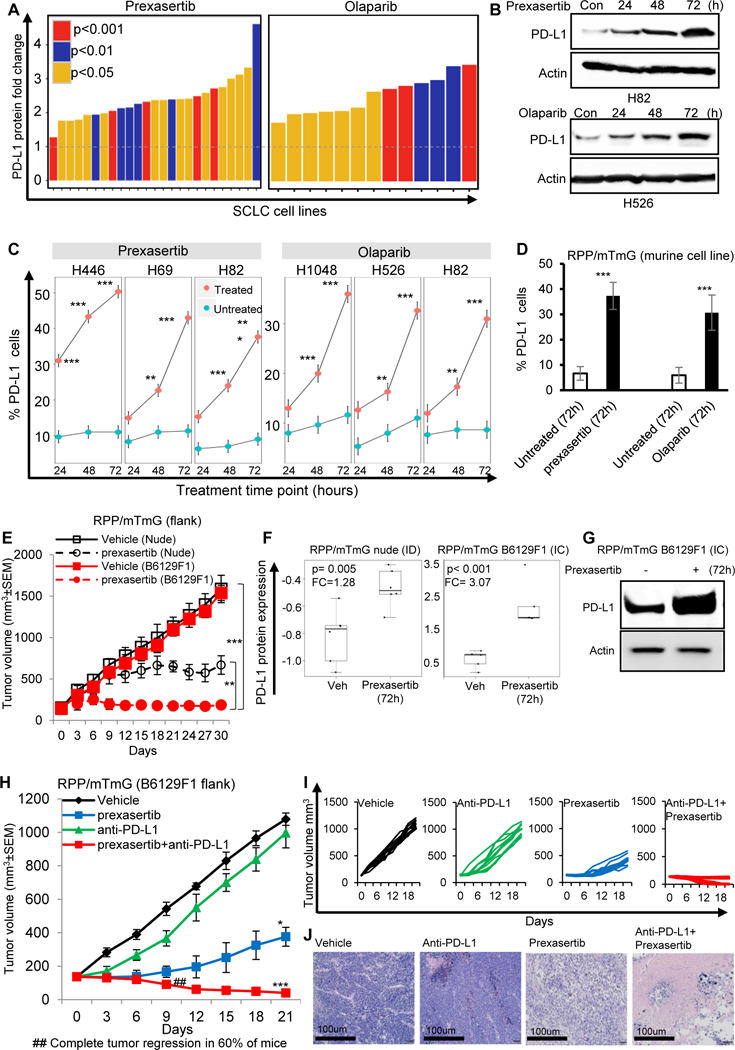
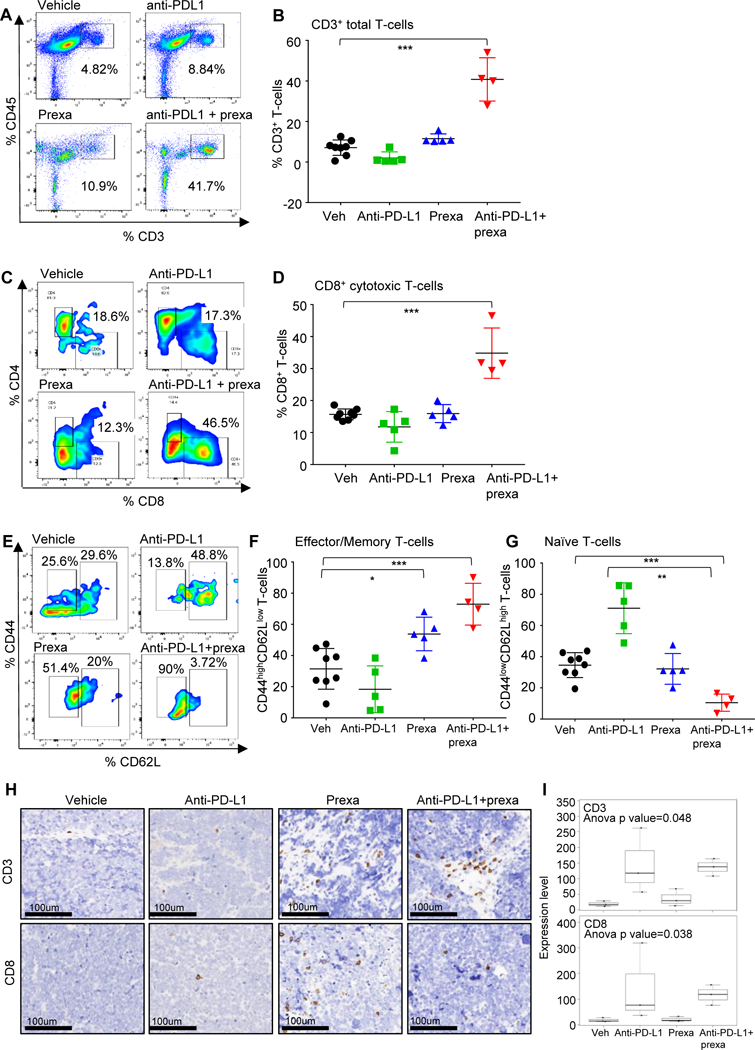
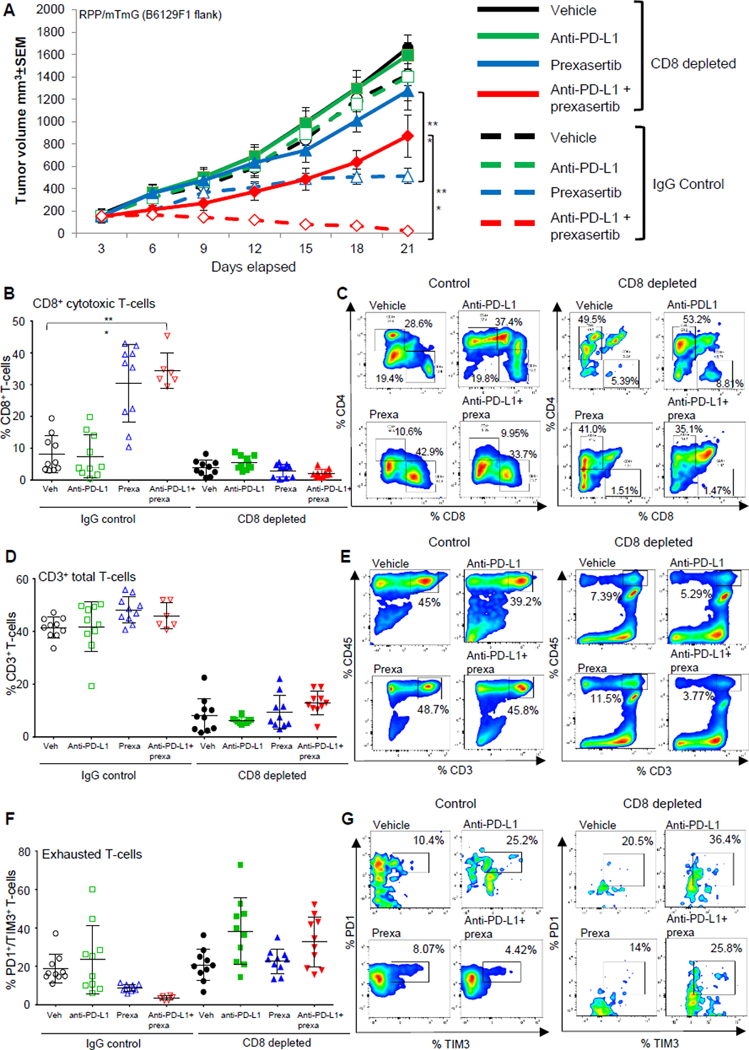
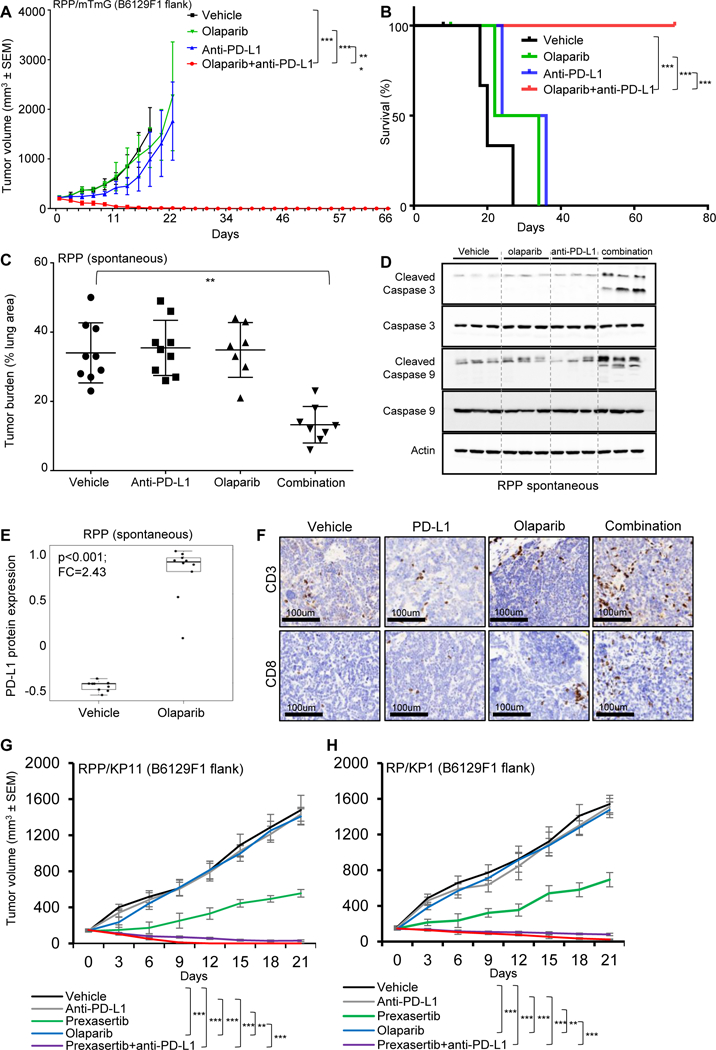
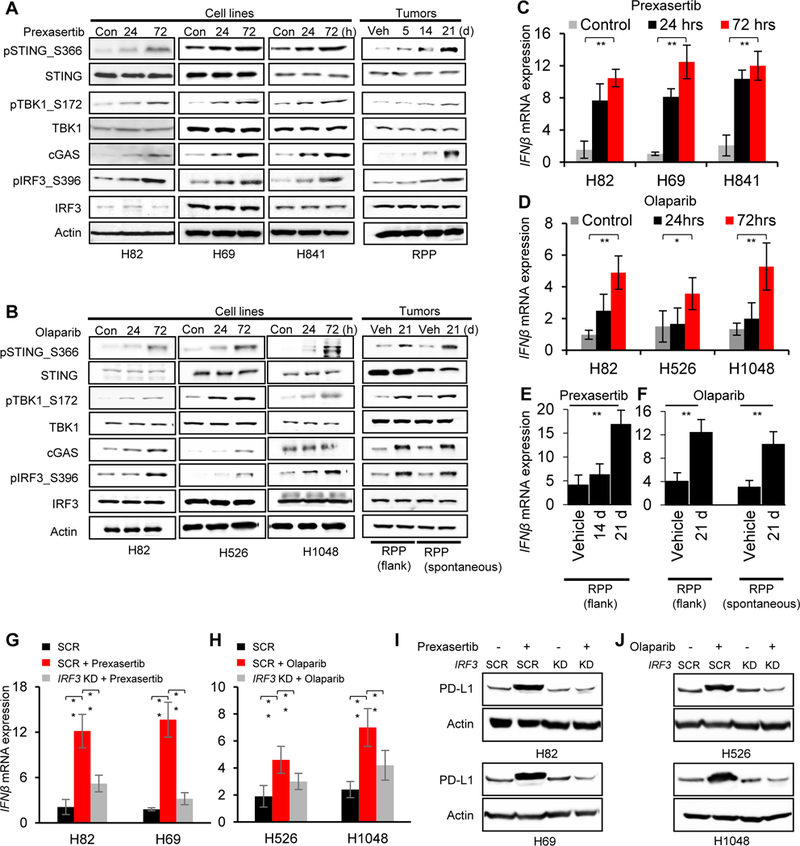
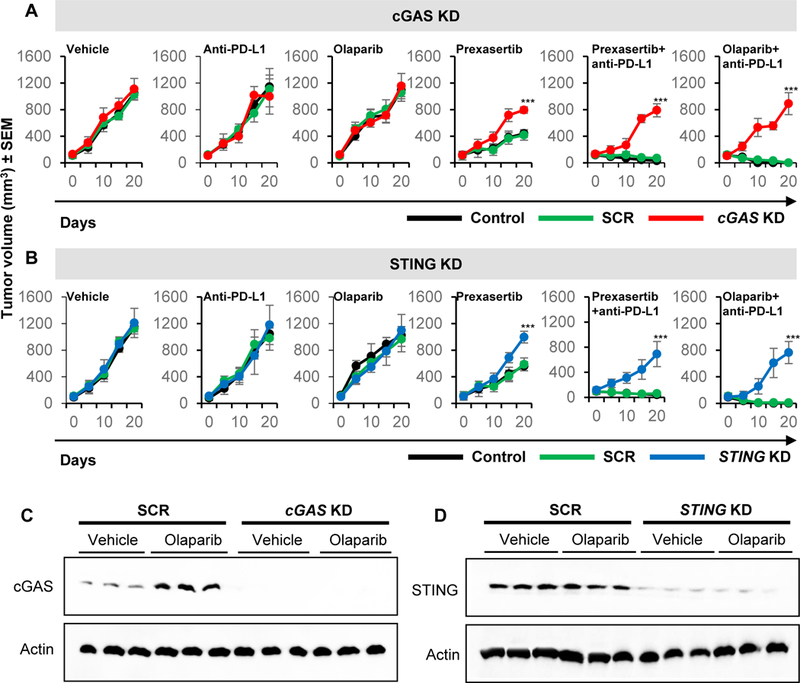
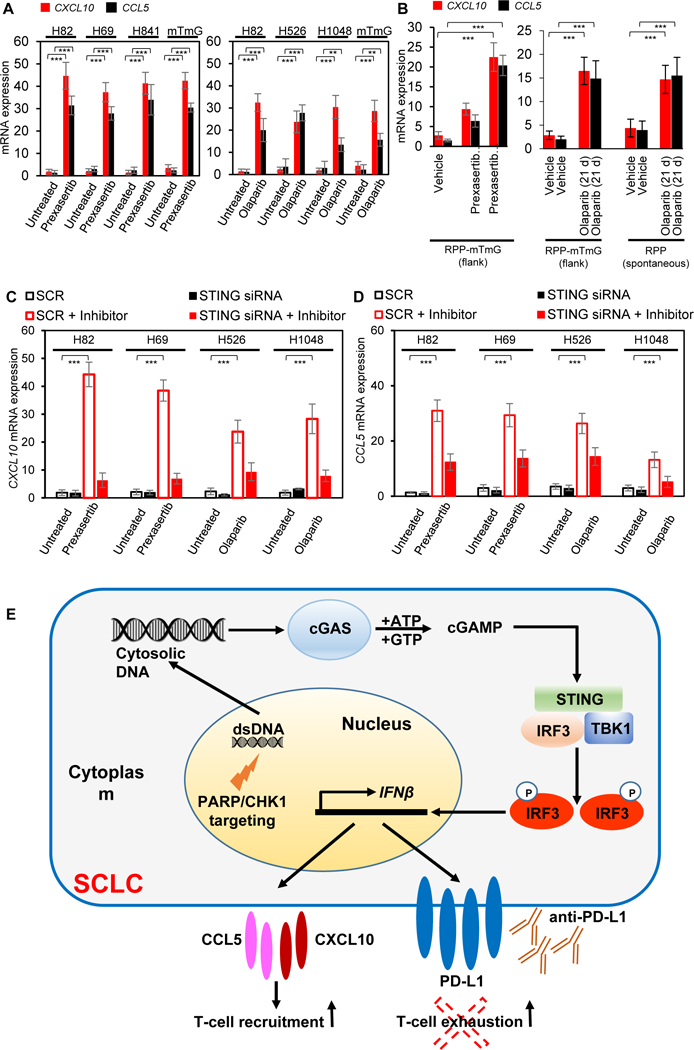
Despite recent advances in the use of immunotherapy, only a minority of patients with small cell lung cancer (SCLC) respond to immune checkpoint blockade (ICB). Here, we show that targeting the DNA damage response (DDR) proteins PARP and checkpoint kinase 1 (CHK1) significantly increased protein and surface expression of PD-L1. PARP or CHK1 inhibition remarkably potentiated the antitumor effect of PD-L1 blockade and augmented cytotoxic T-cell infiltration in multiple immunocompetent SCLC in vivo models. CD8+ T-cell depletion reversed the antitumor effect, demonstrating the role of CD8+ T cells in combined DDR-PD-L1 blockade in SCLC. We further demonstrate that DDR inhibition activated the STING/TBK1/IRF3 innate immune pathway, leading to increased levels of chemokines such as CXCL10 and CCL5 that induced activation and function of cytotoxic T lymphocytes. Knockdown of cGAS and STING successfully reversed the antitumor effect of combined inhibition of DDR and PD-L1. Our results define previously unrecognized innate immune pathway-mediated immunomodulatory functions of DDR proteins and provide a rationale for combining PARP/CHK1 inhibitors and immunotherapies in SCLC. SIGNIFICANCE: Our results define previously unrecognized immunomodulatory functions of DDR inhibitors and suggest that adding PARP or CHK1 inhibitors to ICB may enhance treatment efficacy in patients with SCLC. Furthermore, our study supports a role of innate immune STING pathway in DDR-mediated antitumor immunity in SCLC.See related commentary by Hiatt and MacPherson, p. 584.This article is highlighted in the In This Issue feature, p. 565.
©2019 American Association for Cancer Research.
Conflict of interest statement
Conflict of Interest:
Figures
Comment in
-
Unexpected Synergy Reveals New Therapeutic Strategy in SCLC.Trends Pharmacol Sci. 2019 May;40(5):295-297. doi: 10.1016/j.tips.2019.03.005. Epub 2019 Apr 8. Trends Pharmacol Sci. 2019. PMID: 30975441
-
Delivering a STINGing Blow to Small Cell Lung Cancer via Synergistic Inhibition of DNA-Damage Response and Immune-Checkpoint Pathways.Cancer Discov. 2019 May;9(5):584-586. doi: 10.1158/2159-8290.CD-19-0234. Cancer Discov. 2019. PMID: 31043412
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
