

Robotic-assisted surgery for colorectal liver metastasis: A single-centre experience
- PMID: 30777992
- PMCID: PMC7176011
- DOI: 10.4103/jmas.JMAS_265_18
Robotic-assisted surgery for colorectal liver metastasis: A single-centre experience
Abstract
Background: Although minimally invasive surgery (MIS) of the liver is increasingly widespread, its role in the treatment of colorectal liver metastasis (CRLM) remains uncertain. In this setting, the role of robotic-assisted surgery (RAS) has not been significantly evaluated yet. The aim of this study was to report our experience with RAS for treatment of CRLM.
Material and methods: Prospectively collected surgical and oncologic data on all of the robotic-assisted liver resections for CRLM performed at our centre were retrieved from the institutional database and retrospectively analysed. Intra-operative ultrasound (US) was obtained with a dedicated robotic probe using the TilePro™ function.
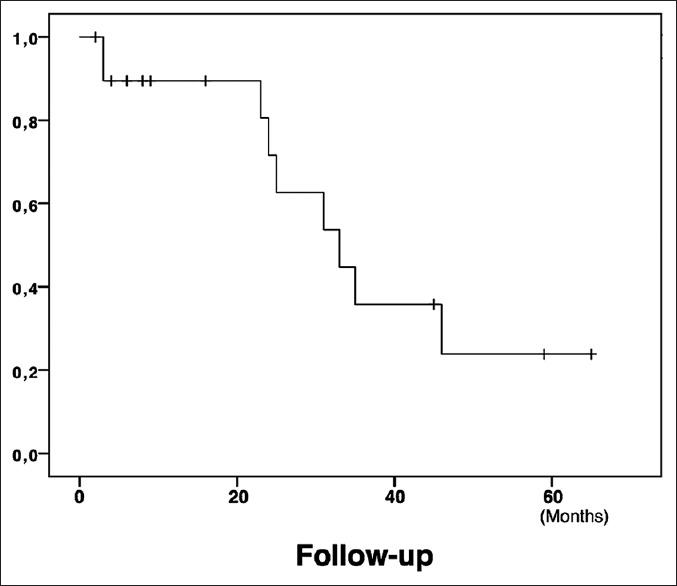
Results: Twenty patients underwent robotic-assisted resection of CRLM between May 2012 and April 2018. Six patients (30%) had multiple synchronous CRLM resections (median = 2; range 2-4). The tumour size averaged 3.0 ± 1.8 cm. All of the lesions were removed using a parenchymal-sparing approach, with R0 resection margins. Mean hospital stay was 4.7 ± 1.8 days. The mean follow-up was 22.5 ± 19.5 months. During the study period, there were no local recurrences, while 9 patients (45%) developed new systemic metastasis. All patients are still alive as of September 2018 with 1- and 3-year disease-free survival of 89.5% and 35.8%, respectively.
Conclusions: In our experience, RAS for CRLM surgical treatment was feasible and played a positive role even in patients with multiple metastases and previous or synchronous surgery. RAS seemed to be oncologically effective in this setting, as no patients experienced local relapse in the treated area.
Keywords: Colorectal metastasis; da Vinci; intra-operative ultrasound; minimally invasive surgery; robotic-assisted.
Conflict of interest statement
None
Figures
References
-
- Julien LA, Thorson AG. Current neoadjuvant strategies in rectal cancer. J Surg Oncol. 2010;101:321–6. - PubMed
-
- Charnsangavej C, Clary B, Fong Y, Grothey A, Pawlik TM, Choti MA, et al. Selection of patients for resection of hepatic colorectal metastases: Expert consensus statement. Ann Surg Oncol. 2006;13:1261–8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous