

Delayed Captopril Administration Mitigates Hematopoietic Injury in a Murine Model of Total Body Irradiation
- PMID: 30778109
- PMCID: PMC6379397
- DOI: 10.1038/s41598-019-38651-2
Delayed Captopril Administration Mitigates Hematopoietic Injury in a Murine Model of Total Body Irradiation
Abstract
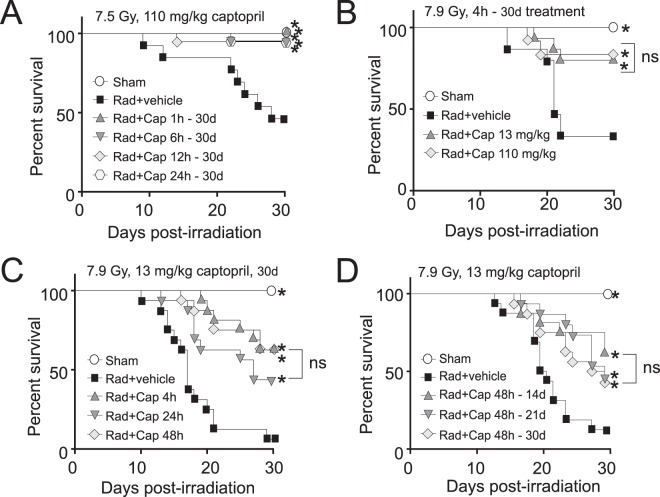
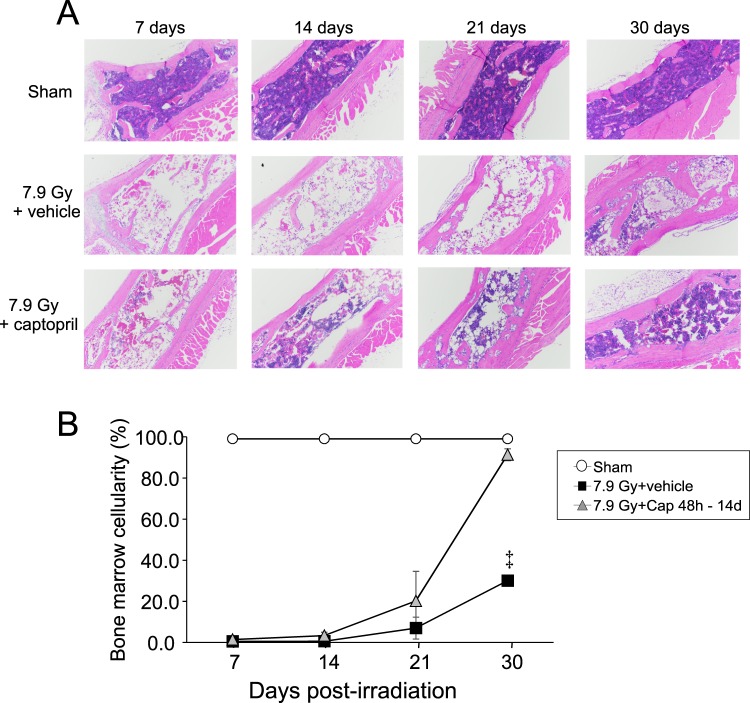
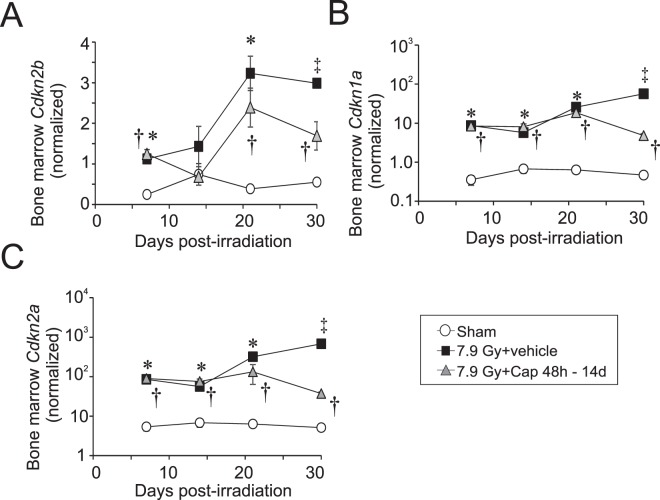
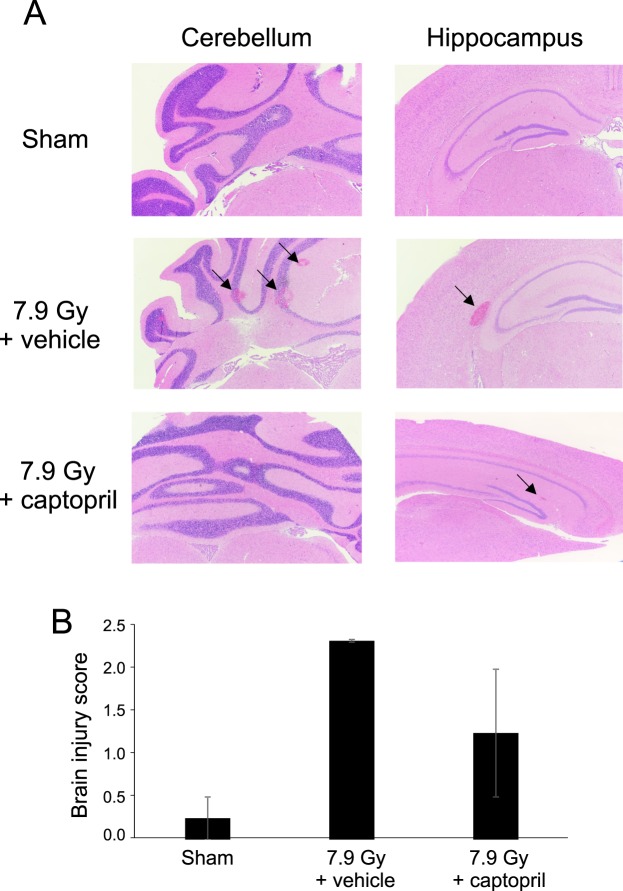
The increasing potential for accidental radiation exposure from either nuclear accidents or terrorist activities has escalated the need for radiation countermeasure development. We previously showed that a 30-day course of high-dose captopril, an ACE inhibitor, initiated 1-4 h after total body irradiation (TBI), improved Hematopoietic Acute Radiation Syndrome (H-ARS) and increased survival in mice. However, because of the time likely required for the deployment of a stockpiled radiation countermeasure to a radiation mass casualty site, there is a need for therapies that can be administered 24-48 hours after initial exposure. Using C57BL/6 mice exposed to an LD50-80/30 of 60Co TBI (7.75-7.9 Gy, 0.615 Gy/min), we show that low-dose captopril administration, initiated as late as 48 h post-TBI and continued for 14 days, significantly enhanced overall survival similarly to high-dose, rapid administration. Captopril treatment did not affect radiation-induced cell cycle arrest genes or the immediate loss of hematopoietic precursors. Reduced mortality was associated with the recovery of bone marrow cellularity and mature blood cell recovery at 21-30 days post-irradiation. Captopril reduced radiation-induced cytokines EPO, G-CSF, and SAA in the plasma. Finally, delayed captopril administration mitigated brain micro-hemorrhage at 21 days post-irradiation. These data indicate that low dose captopril administered as late as 48 h post-TBI for only two weeks improves survival that is associated with hematopoietic recovery and reduced inflammatory response. These data suggest that captopril may be an ideal countermeasure to mitigate H-ARS following accidental radiation exposure.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- U.S. Food & Drug Administration. Radiological and nuclear emergency preparedness information from FDA, https://www.fda.gov/EmergencyPreparedness/Counterterrorism/MedicalCounte... (2018).
-
- Meder J, Michalowski A. Changes in cellularity and/or weight of mouse hemopoietic tissues as a measure of acute radiation effects. Arch Immunol Ther Exp (Warsz). 1980;28:9–18. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
