

Risk of Pneumonitis and Pneumonia Associated With Immune Checkpoint Inhibitors for Solid Tumors: A Systematic Review and Meta-Analysis
- PMID: 30778352
- PMCID: PMC6369169
- DOI: 10.3389/fimmu.2019.00108
Risk of Pneumonitis and Pneumonia Associated With Immune Checkpoint Inhibitors for Solid Tumors: A Systematic Review and Meta-Analysis
Abstract
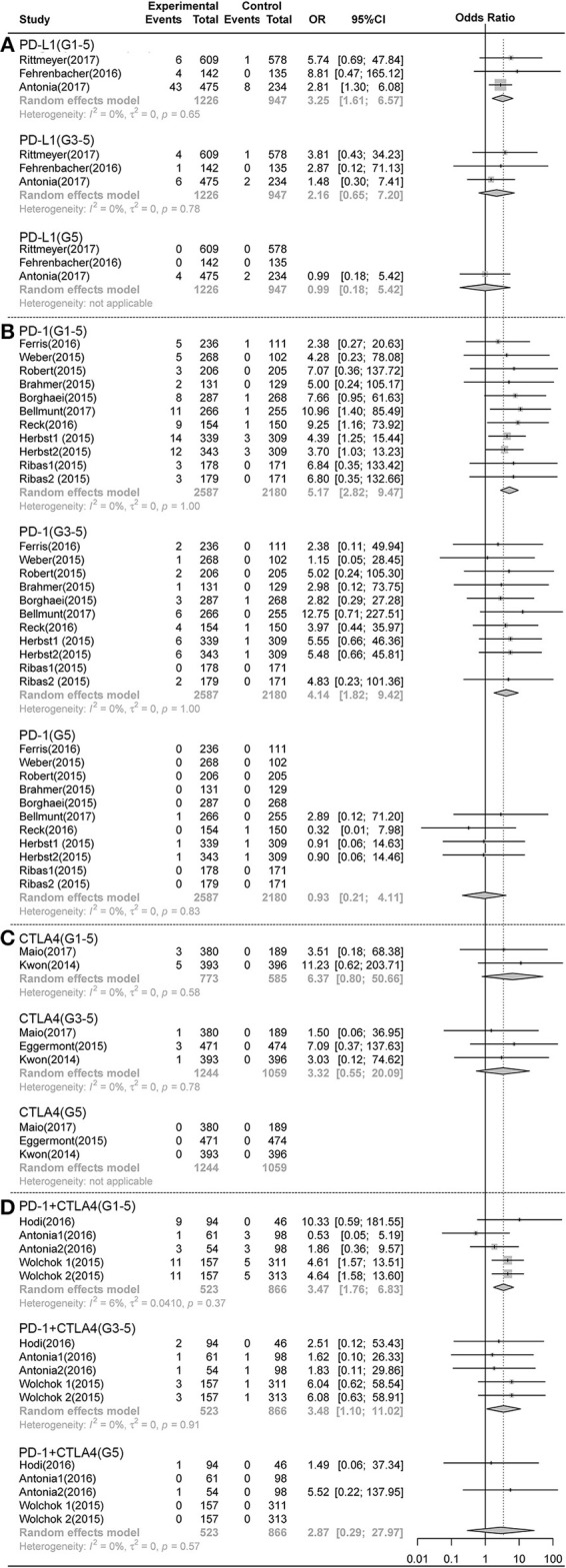
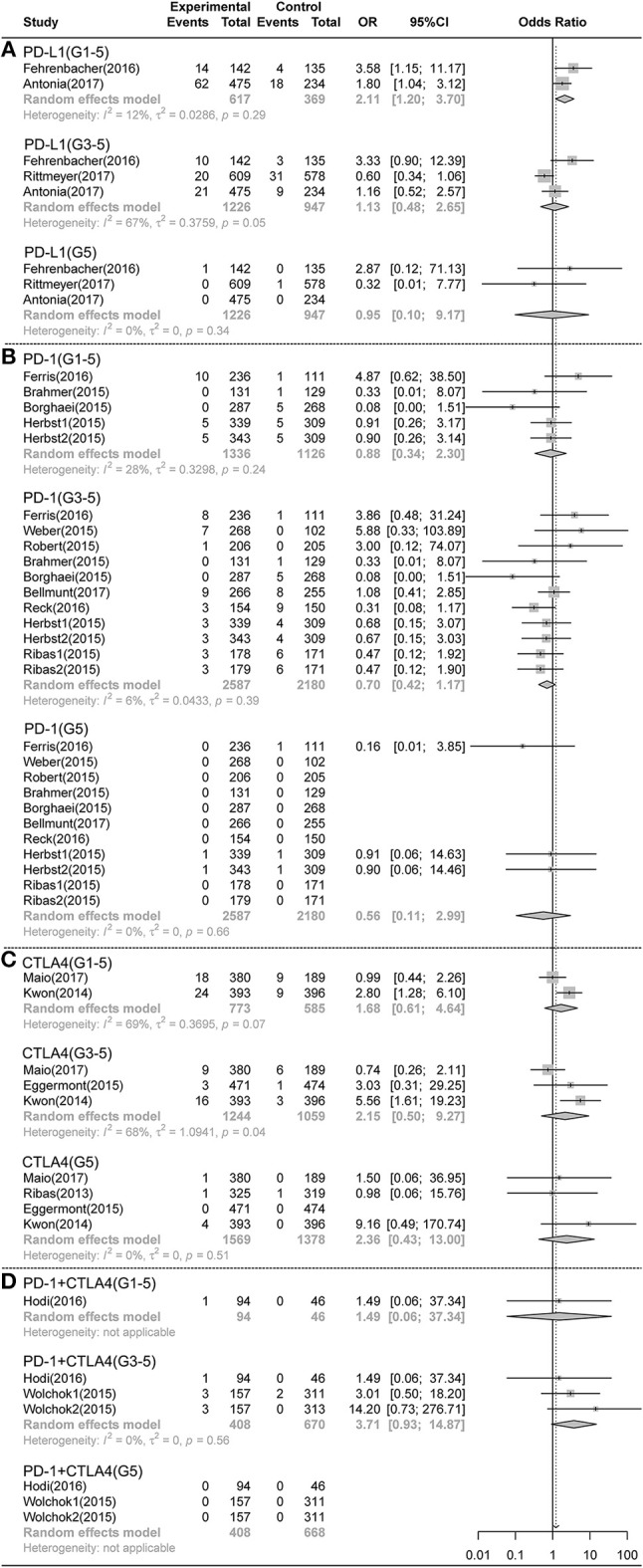
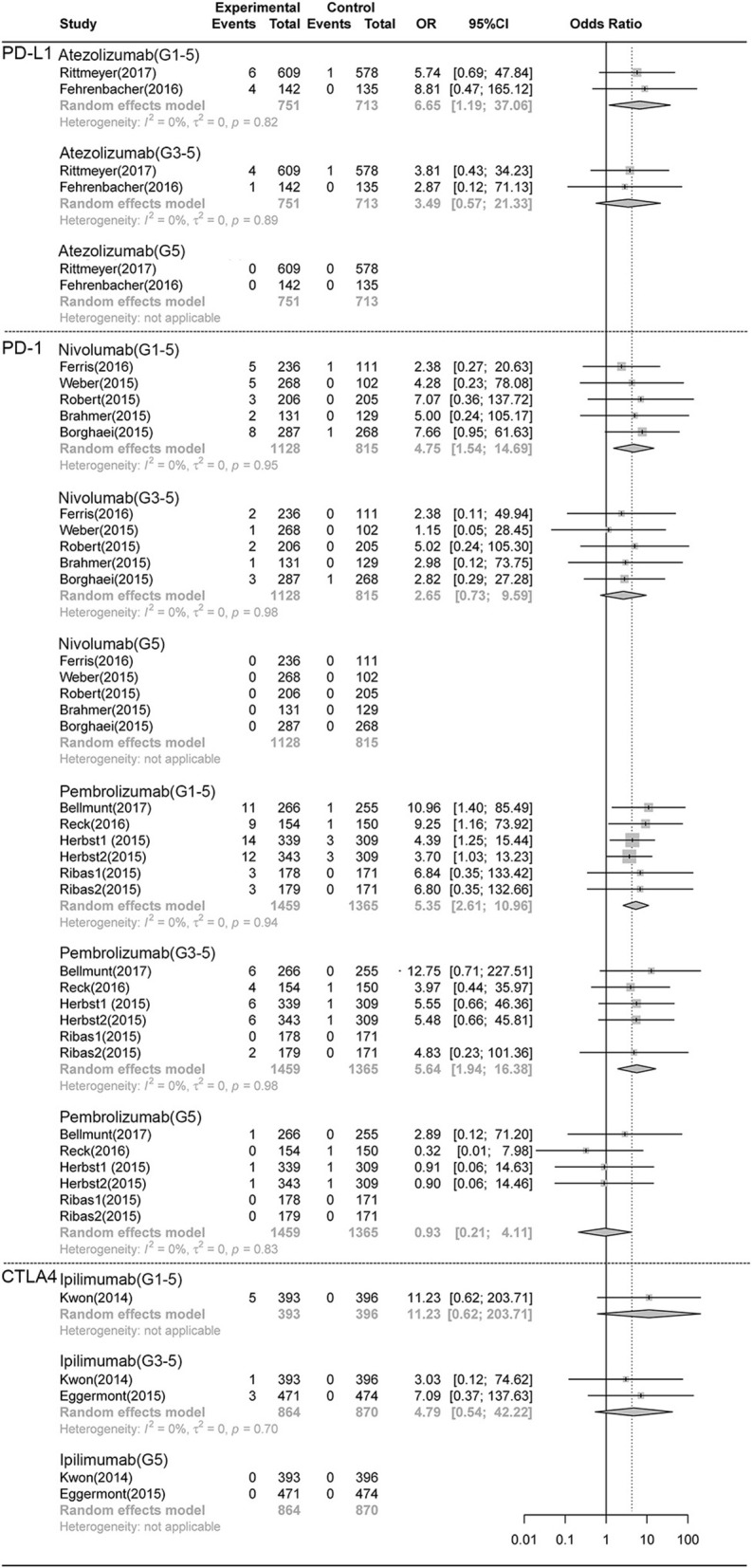
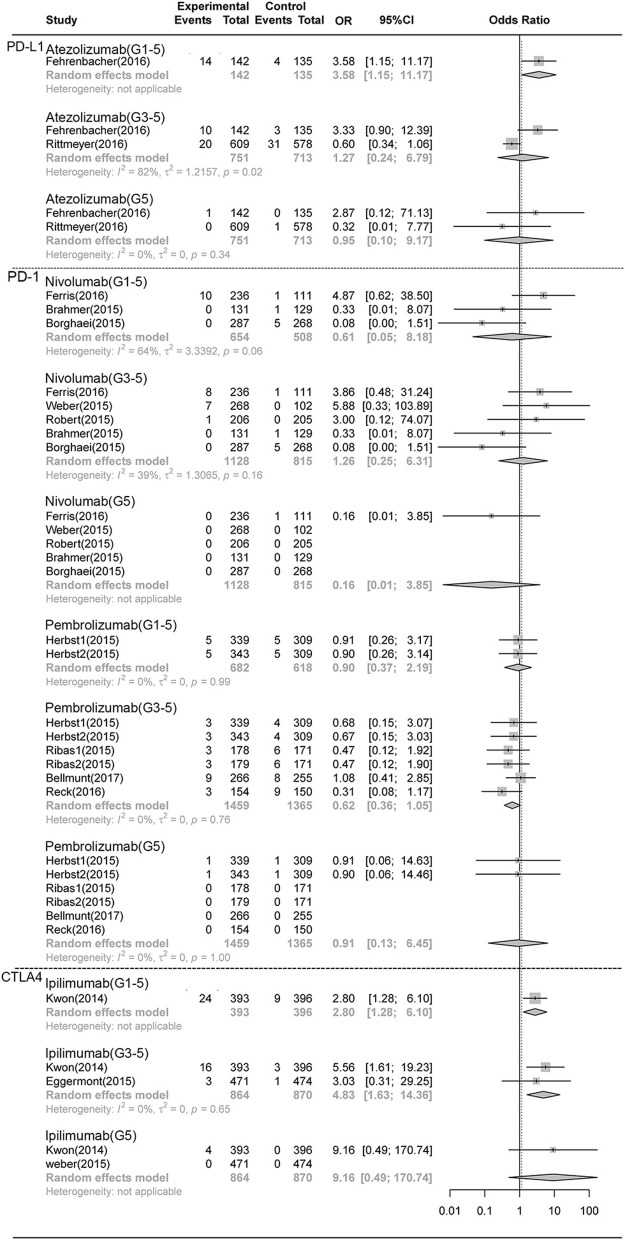
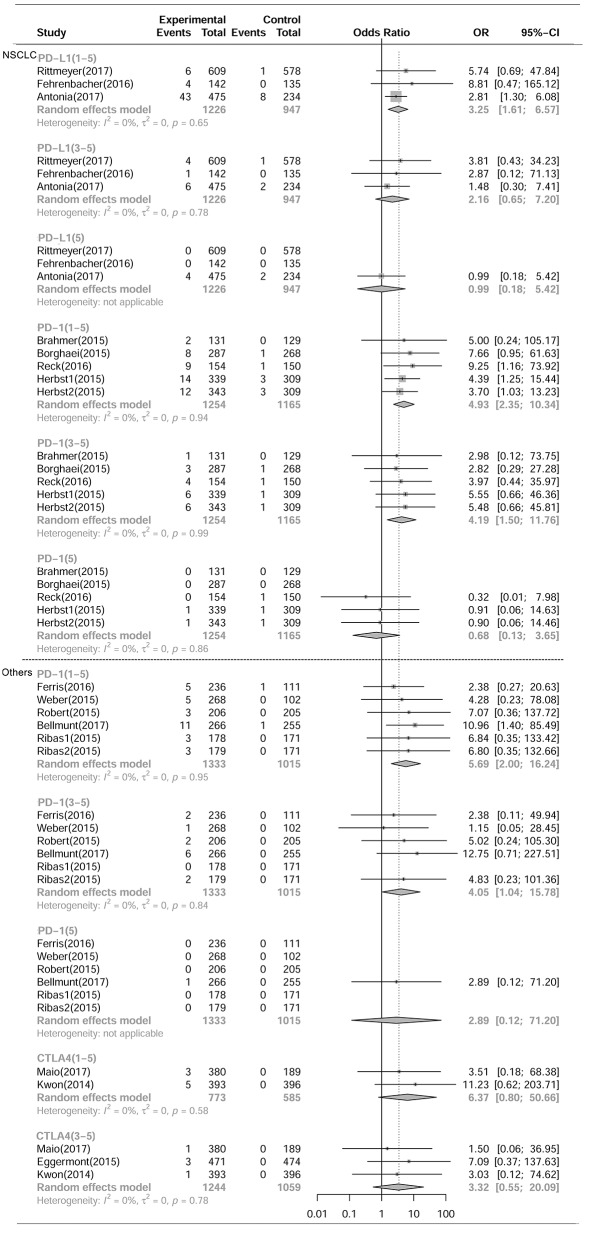
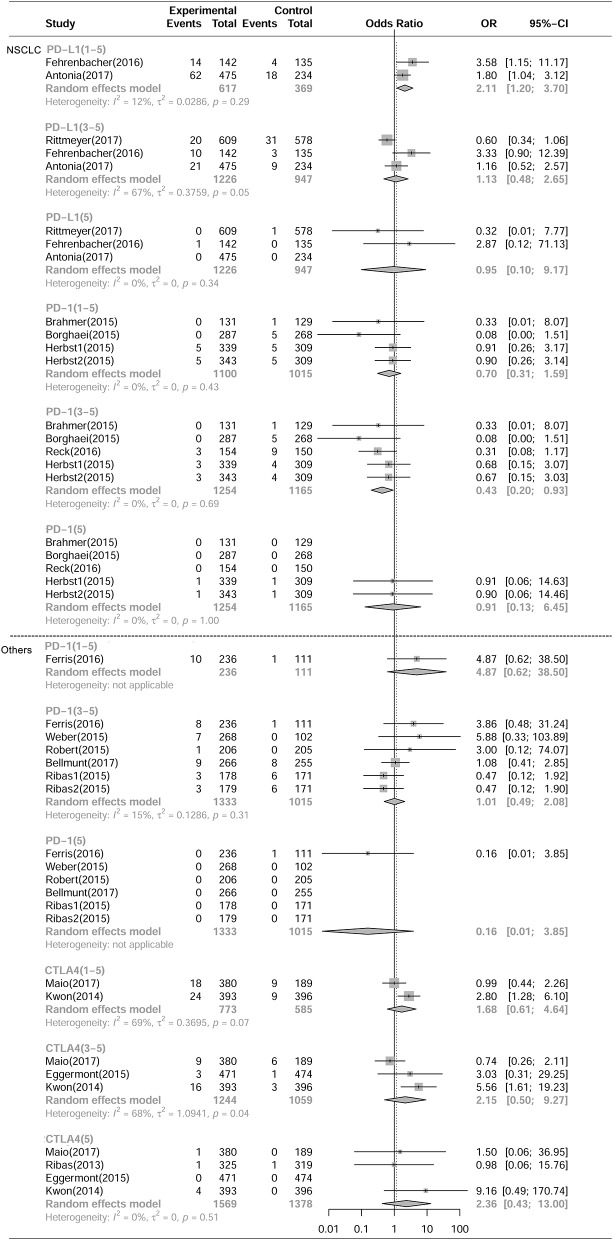
Background: We performed a systematic review and meta-analysis to evaluate the risk of pneumonitis and pneumonia associated with immune checkpoint inhibitors (ICIs) for solid tumors. Methods: The following keywords were used in searching the Embase and PubMed database: pneumonitis, pneumonia, and immune checkpoint inhibitors. The data was analyzed by using the R software and Metafor package. Results: Among 3,436 studies, 23 randomized clinical trials (RCTs) met our selection criteria which included data from 12,876 patients. Compared with chemotherapy, PD-1 inhibitors showed significant increase in grade 1-5 and grade 3-5 pneumonitis (RR, 5.17, 95% CI: 2.82-9.47, p < 0.001; RR, 4.14, 95% CI: 1.82-9.42, p < 0.001), but not in pneumonia. PD-L1 inhibitors showed significant increase in grade 1-5 pneumonitis and pneumonia (RR, 3.25, 95% CI: 1.61-6.57, p < 0.001; RR, 2.11, 95% CI: 1.20-3.70, p < 0.001). There was no significant difference in any grade pneumonitis and pneumonia in cytotoxic T lymphocyte-associated protein 4 (CTLA4) inhibitors subgroup. Programmed cell death protein 1 (PD-1) inhibitor (nivolumab and pembrolizumab) both showed significant increase in grade 1-5 pneumonitis, and pembrolizumab specially tended to increase grade 3-5 pneumonitis. (RR, 5.64 95% CI: 1.94-16.38, p < 0.001). Compared with PD-1 inhibitor (nivolumab) or CTLA-4 inhibitor (ipilimumab) monotherapy, PD-1 inhibitor, and CTLA-4 inhibitor (nivolumab plus ipilimumab) combination therapies showed significant increase in grade 1-5 and grade 3-5 pneumonitis (RR 3.47, 95%CI:1.76-6.83, p < 0.001; RR 3.48, 95%CI: 1.10-11.02, p < 0.001). Conclusions: PD-1/PD-L1 inhibitors treatment could increase the risk of all-grade pneumonitis. CTLA4 inhibitor ipilimumab treatment alone could not increase the risk of pneumonitis but could augment the risk of pneumonitis in PD-1/PD-L1 inhibitor treated patients. There was no significant increase in the risk of pneumonia after either PD-1/PDL-1inhibitor or CTLA4 inhibitor treatment alone or in combination.
Keywords: immune checkpoint inhibitors; meta-analysis; pneumonia; pneumonitis; solid tumour.
Figures
References
-
- Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, von Pawel J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet (2017) 389:255–65. 10.1016/S0140-6736(16)32517-X - DOI - PMC - PubMed
-
- Fehrenbacher L, Spira A, Ballinger M, Kowanetz M, Vansteenkiste J, Mazieres J, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet (2016) 387:1837–46. 10.1016/S0140-6736(16)00587-0 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous