

The outcomes of total knee arthroplasty in morbidly obese patients: a systematic review of the literature
- PMID: 30778723
- PMCID: PMC6420900
- DOI: 10.1007/s00402-019-03127-5
The outcomes of total knee arthroplasty in morbidly obese patients: a systematic review of the literature
Abstract
Introduction: The increasing prevalence of obesity has led to an increase in total knee arthroplasties (TKAs) being undertaken in patients with a higher body mass index (BMI). TKA in morbidly obese patients can be technically challenging due to numerous anatomical factors and patient co-morbidities. The long-term outcomes in this patient group are unclear. This systematic review aims to compare the long-term revision rates, functional outcomes and complication rates of TKAs in morbidly obese versus non-obese patients.
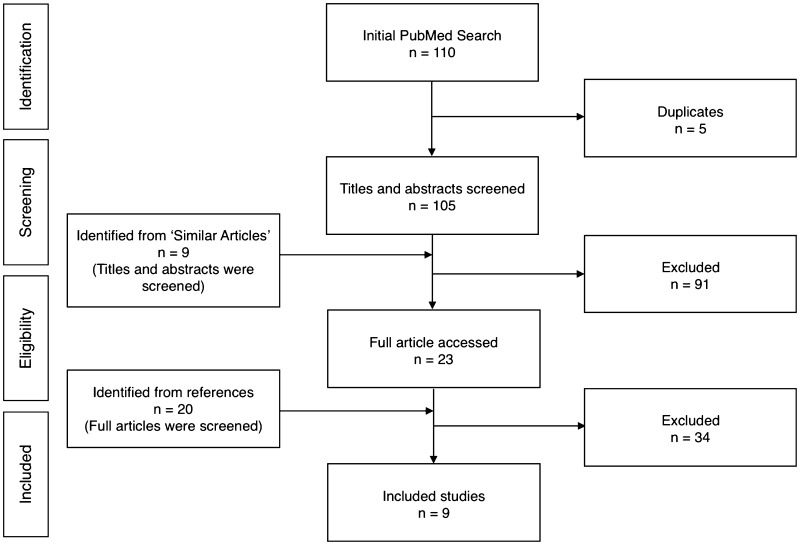
Methods: A search of PubMed, EMBASE and PubMed Central was conducted to identify studies that reported revision rates in a cohort of morbidly obese patients (BMI ≥ 40 kg/m2) that underwent primary TKA, compared to non-obese patients (BMI ≤ 30 kg/m2). Secondary outcomes included Knee Society Objective Scores (KSOS), Knee Society Functional Scores (KSFS), and complication rates between the two groups. The difference in revision rates was assessed using the Chi-squared test. The Wilcoxon signed-rank test was used to compare pre-operative and post-operative functional scores for each group. KSOS and KSFS for morbidly obese and non-obese patients were compared using the Mann-Whitney test. Statistical significance was defined as p ≤ 0.05.
Results: Nine studies were included in this review. There were 624 TKAs in morbidly obese patients and 9,449 TKAs in non-obese patients, average BMI values were 45.0 kg/m2 (range 40-66 kg/m2) and 26.5 kg/m2 (range 11-30 kg/m2) respectively. The average follow-up time was 4.8 years (range 0.5-14.1) and 5.2 years (range 0.5-13.2) respectively, with a revision rate of 7% and 2% (p < 0.001) respectively. All functional scores improved after TKA (p < 0.001). Pre- and post-operative KSOS and KSFS were poorer in morbidly obese patients, however, mean improvement in KSOS was the same in both groups and comparable between groups for KSFS (p = 0.78). Overall complication rates, including infection, were higher in morbidly obese patients.
Conclusions: This review suggests an increased mid to long-term revision rate following primary TKA in morbidly obese patients, however, these patients have a functional recovery which is comparable to non-obese individuals. There is also an increased risk of perioperative complications, such as superficial wound infection. Morbidly obese patients should be fully informed of these issues prior to undergoing primary TKA.
Keywords: Complication rates; Complications; Functional outcome; Infection; Infection rates; KSFS; KSOS; Knee Society Functional scores; Knee Society Objective scores; Morbid obesity; Non-obese; Obesity; Prosthetic infection; Quality of life; Revision rate; Superficial wound infection; TKA; TKR; Total knee arthroplasty; Total knee replacement; Wound healing delay; Wound healing problems.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Green M, Howard P, Porter M, Wilkinson M, Wishart N, Porteus M et al. (2017) NJR 14th Annual Report. Natl Jt Regist 14th Annu Rep.
-
- Culliford D, Maskell J, Judge A, Cooper C, Prieto-Alhambra D, Arden NK. Future projections of total hip and knee arthroplasty in the UK: results from the UK Clinical Practice Research Datalink. Osteoarthr Cartil. 2015;23(4):594–600. - PubMed
-
- Wang YC, McPherson K, Marsh T, Gortmaker SL, Brown M. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet. 2011;378(9793):815–825. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
