

Review
doi: 10.1007/s40477-018-0352-z.
Epub 2019 Feb 18.
Paediatric liver ultrasound: a pictorial essay
Affiliations
- PMID: 30778891
- PMCID: PMC7010916
- DOI: 10.1007/s40477-018-0352-z
Item in Clipboard
Review
Paediatric liver ultrasound: a pictorial essay
J Ultrasound.
2020 Mar.
Abstract
Ultrasound scan is a painless and radiation-free imaging modality and, therefore, it is widely considered the first-choice diagnostic tool in the setting of hepatopathies in paediatric patients. This article focuses on the normal ultrasound anatomy of the liver in neonatal and paediatric age and reviews the ultrasound appearance of the most common diffuse and focal liver affections.
Keywords: Cholestasis; Diffuse hepatopathies; Focal liver lesions; Liver; Paediatric; Ultrasound.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
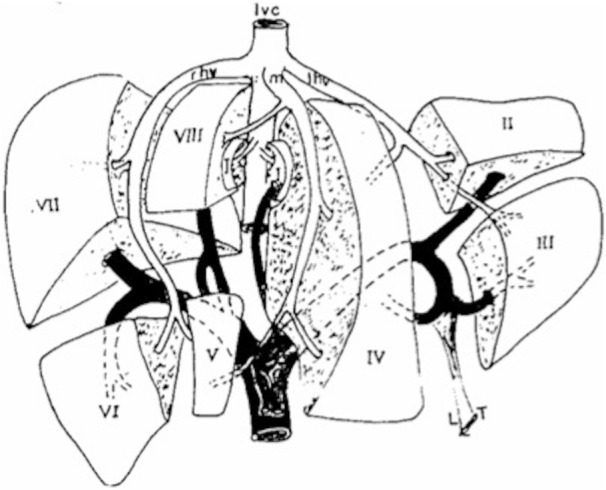
Schematic overview of segmental anatomy of the liver. Commonly, segments are identified following portal and venous branches ramifications
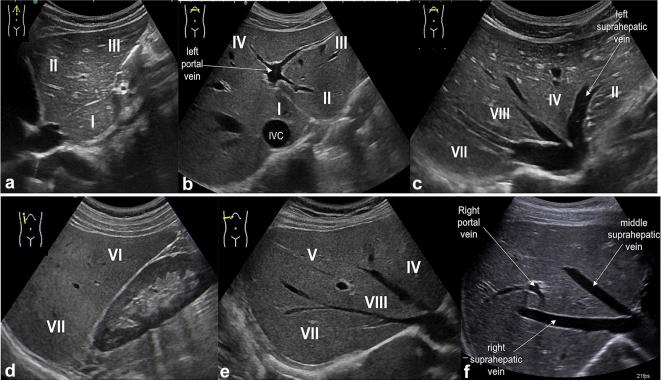
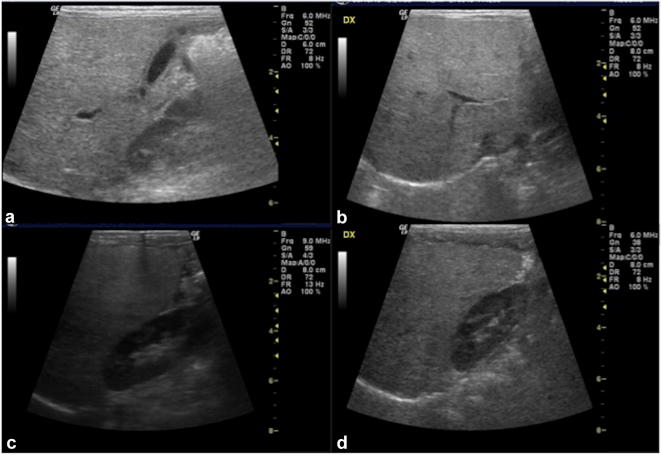
US study of the liver: longitudinal and transverse scan along the midline (a, b) show the left hepatic lobe (segments II and III) separated from segment I (close to the inferior vena cava, IVC) and the left portal vein with its feeding branches for segments II, III and IV; in the oblique subcostal scan (c) there are right, middle and left hepatic veins which separate segments VII, VIII, IV and II; longitudinal scan along hemiclavear line (d) shows segments VII and VI; oblique subcostal scans (e, f) show right portal vein separating segments VIII and V
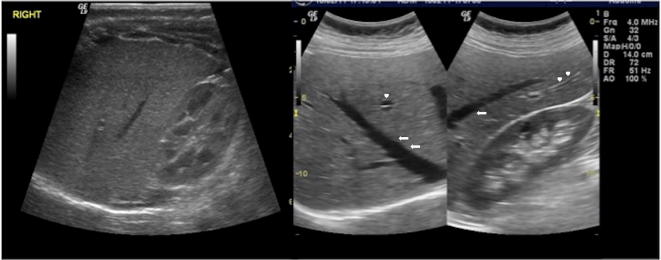
US study of the liver, longitudinal and oblique scans: normal hepatic echostructure is characterised by homogenous low-to-intermediate echoes similar to the adjacent renal cortex; there are also tubular anechoic structures representing intrahepatic veins (arrows) and portal vein branches (arrowheads)
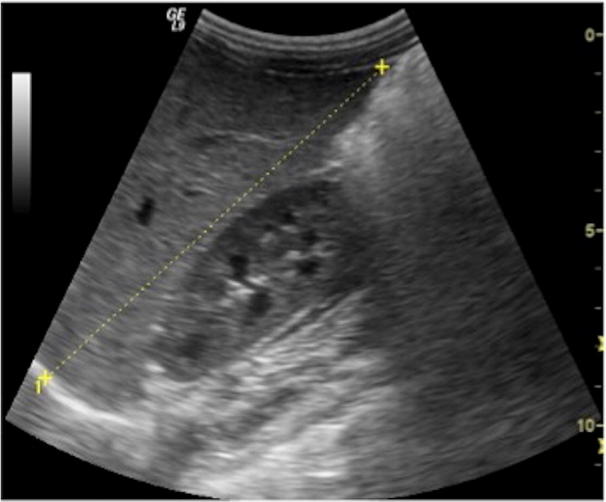
US study of the liver: longitudinal scan along the right hemiclavear line is commonly used to measure the longitudinal diameter of the right hepatic lobe
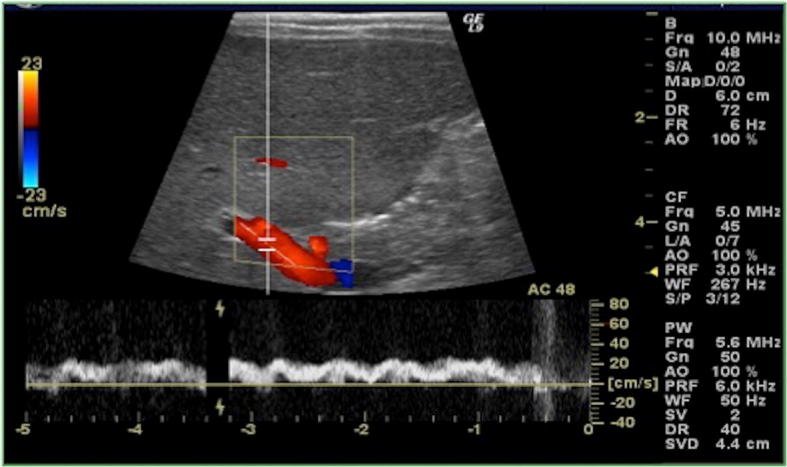
US of the liver, colour-Doppler study of the portal vein at the hilum. Portal flow is usually directed towards the liver, with normal mean velocity of 15–18 cm/s
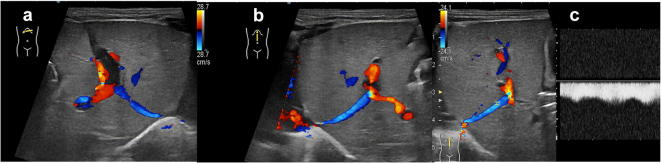
US of the liver with colour-Doppler (a, b) and colour-pulse-Doppler (c) study in a newborn depicts patent ductus venosus (with hepatofugal flow in blue)
US of the liver, oblique scan in patient affected by acute hepatitis: there is an increase of hepatic volume and slight decrease of echostructure, while portal branches wall appears brighter
US of the liver, longitudinal and oblique scans (a–d): the echogenicity of the liver is particularly bright, especially when compared to the adjacent renal cortex (c, d); moreover, there is blurred appearance of intrahepatic vessels walls and loss of diaphragmatic profile

US of the liver, longitudinal, axial and oblique scan: there is hyperechogenic liver parenchyma (particularly when compared to the cortex of right kidney) with quite well-defined area of relatively hypoechogenicity (a, b) due to fat sparing-area; in the right figure (c) there is a geometrical shaped bright area which does not cause any mass effect and is therefore in keeping with focal hepatic steatosis
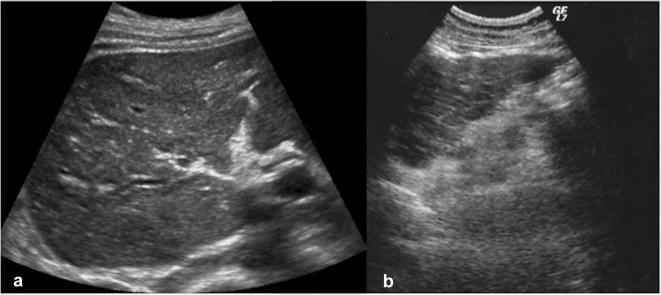
Abdominal US study shows changes in hepatic cirrhosis, with evidence of volume decrease of the right lobe, irregular margins and roughly heterogeneous echogenicity (coarse pattern) in the right (a) and left lobe (b)
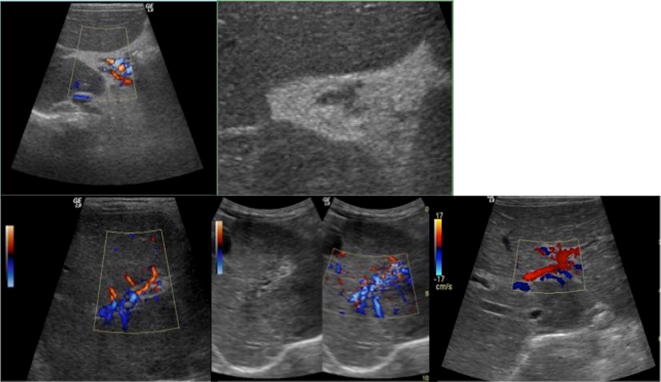
US evaluation in cirrhotic liver with colour-Doppler study: at the hilum, the portal vein is replaced by portal cavernoma, composed by many small tortuous vessels as consequence of portal hypertension and vein thrombosis
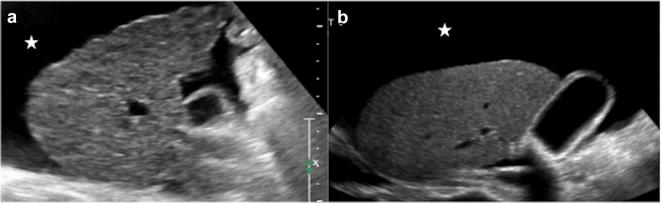
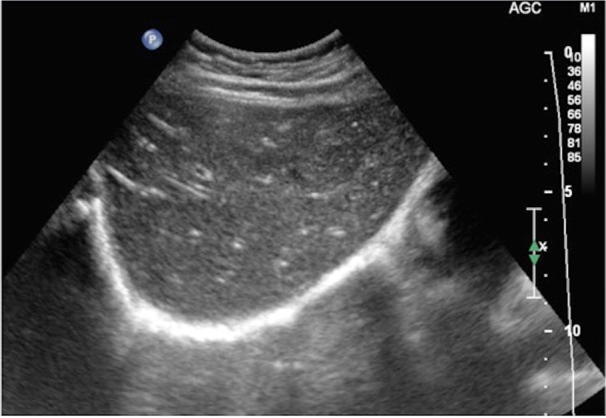
Abdominal US in advanced cirrhotic condition shows hepatic changes do to regeneration process and fibrosis (a, b), with also ascites, that is identified as anechoic fluid around the perihepatic space (star)
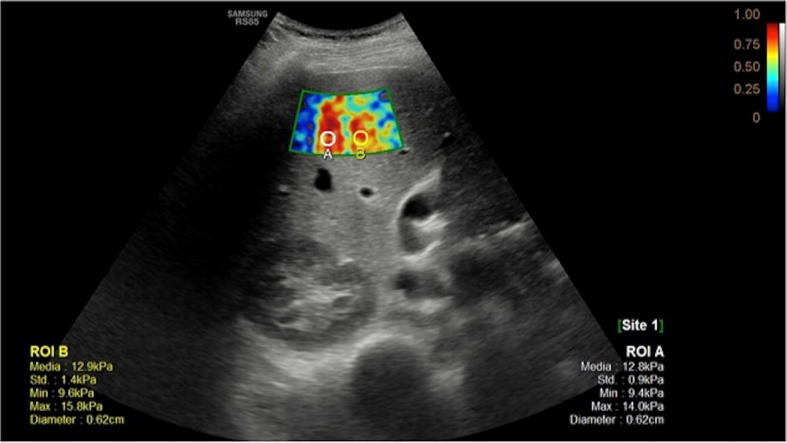
Elastography of cirrhotic liver allows to evaluate stiffness of the parenchyma, which is related to the degree of fibrosis, as it affects the wave velocity measured by the probe

US study of the liver in patient with cystic fibrosis shows diffuse echostructure changes with alternation of hypoechoic and hyperechoic areas
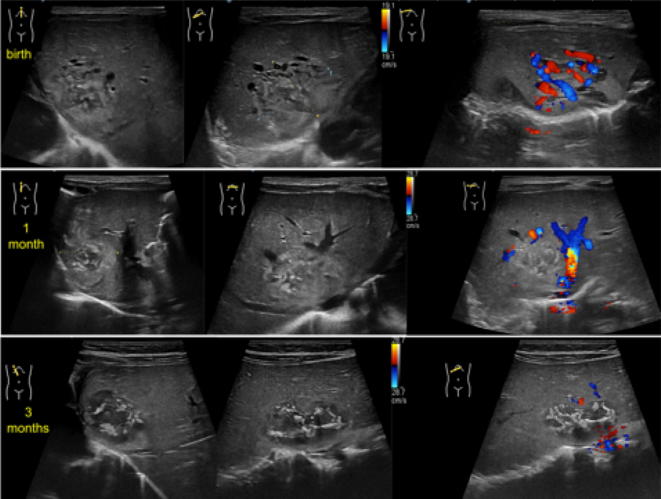
US of the liver, oblique B-Mode imaging and colour-Doppler study at birth (upper line), at 1 month (central line) and at 3 months (lower line): there is a large heterogeneous mass, measuring about 20 mm, mostly iso-hypo-echoic, with internal anechoic tubular structures. Colour-Doppler images shows internal vessels characterised by both arterial and venous flow. At follow-up, B-mode evaluation shows slight reduction of diameter with increase of the internal anechoic necrotic component. Moreover, colour-Doppler tool demonstrates significant reduction and finally disappearing of internal vascular flow. These features were in keeping with the diagnosis of focal hepatic haemangioma

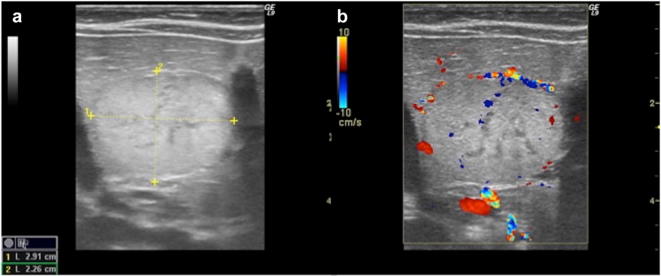
US study of the liver, longitudinal and transverse B-mode images (a, b) and longitudinal colour-Doppler scans (c): there is a well-defined large mass, mostly iso-echoic, showing internal and peripheral vascular flow at colour-Doppler study. This latter takes a spoke-wheel-like appearance which is typical for focal nodular hyperplasia
US study of hepatic adenoma with B-mode and colour-Doppler images: there is a well-defined large hyperechoic mass, with some internal anechoic areas, which shows peripheral and internal vessels (a, b)
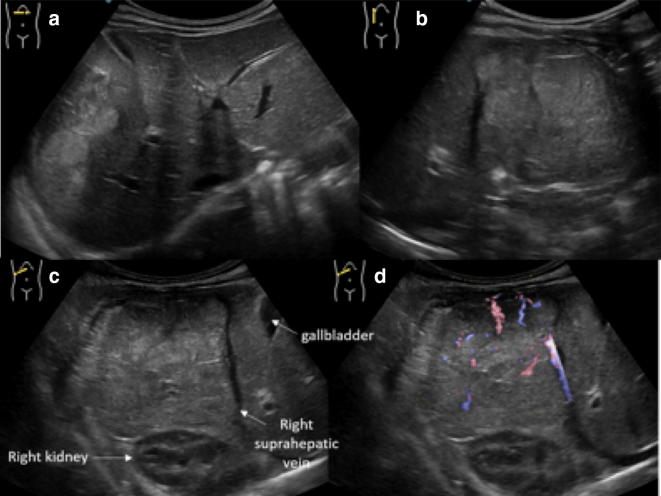
Ultrasonographic images of hepatic hepatoblastoma: there is an ill-defined heterogeneous mass, involving almost completely the right lobe, which shows hyper- and isoechoic areas (a–c); many internal vessels are identified at colour-Doppler image (d)
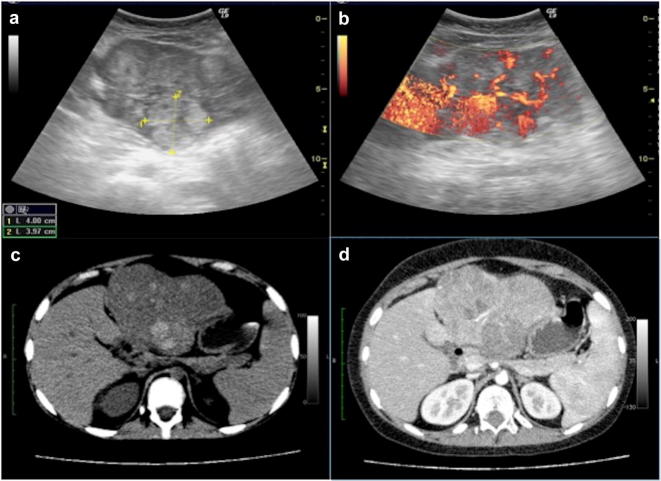
Hepatocarcinoma at US B-Mode and Doppler images (a, b) and axial computed tomography and contrast-enhanced computed tomography images (c, d). At US the tumour appears as large heterogeneous lesion that bulges the liver surface, with significant internal vascular flow (a, b). Computed tomography images show large lesion with hyperdense components at un-enhanced scan (c), which demonstrates heterogeneous enhancement (d)

US study (a, b) and computed tomography axial scans venous phase (c) of amoebic abscess: there is a large well-defined lesion involving VII/VIII segments, which shows internal hypo and anechoic areas at US. Computed tomography scans demonstrates internal fluid component with only enhancement of the irregularly thick peripheral wall
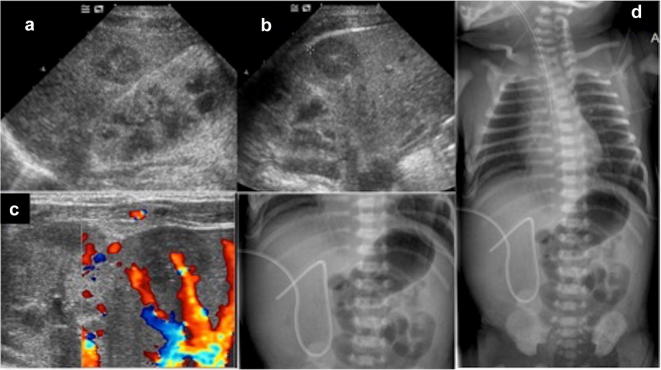
US study of the liver demonstrates the presence of roundish hypo- anechoic area, probably due to parenchymal hematoma caused by displaced UVC (a–c). Frontal abdominal radiography of a newborn showing the UVC ending at the level of right portal vein (d)
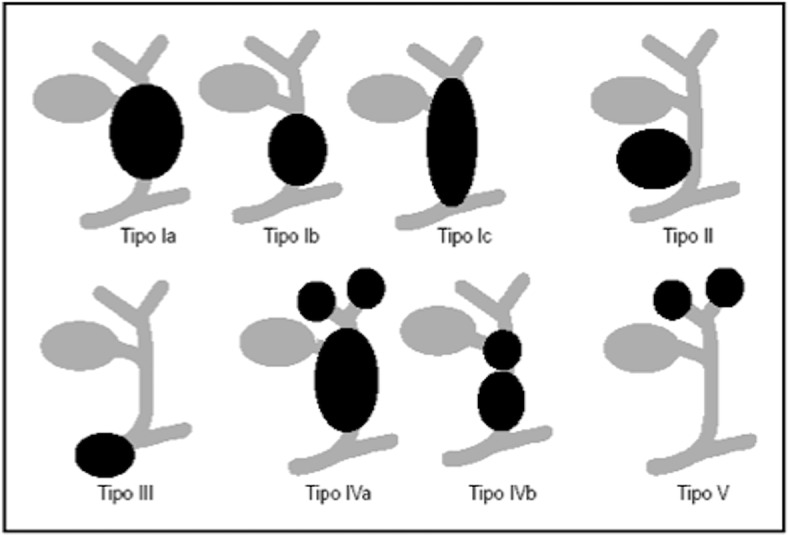
Schematic overview of choledochal cyst (Todani’s classification) Modified from Soares et al. [44]
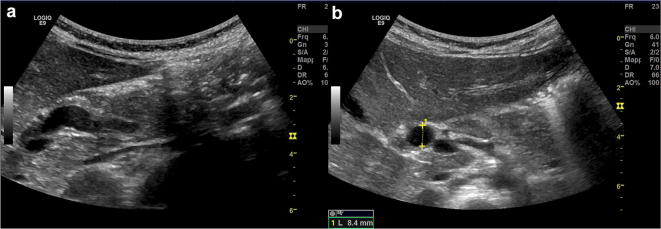
US study of choledochal cyst type I shows fusiform dilatation (a) of extrahepatic bile duct measuring 8.4 mm (b)

US study of the liver with B-mode (a) and colour-Doppler (b) in a newborn with biliary atresia shows hyperechoic tissue (arrows) just near to the hepatic hilum
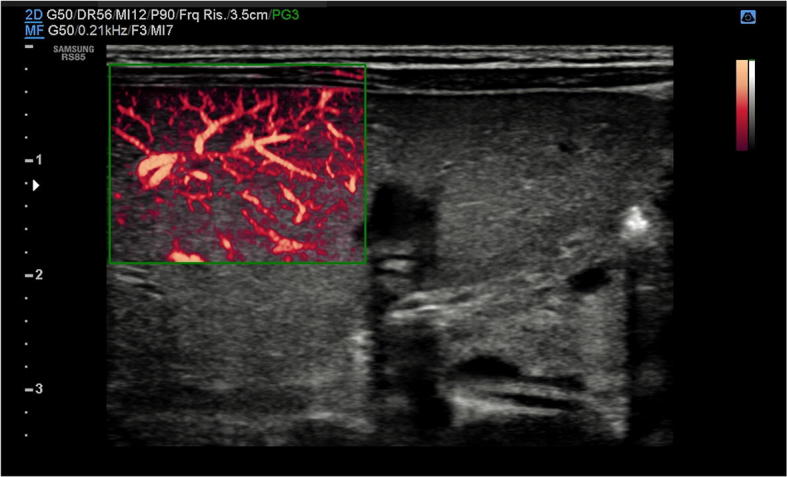
US study of the liver with B-Mode and power Doppler modalities in a newborn with biliary atresia: there is hepatic arterial flow extending to the hepatic surface (subcapsular flow)
Similar articles
-
Focal liver diseases in neonatal and pediatric liver transplant candidates: a pictorial essay.Clin Transplant. 2010 Sep-Oct;24(5):592-8. doi: 10.1111/j.1399-0012.2009.01139.x. Clin Transplant. 2010. PMID: 19888996 Review.
-
[Liver ultrasound: focal lesions and diffuse diseases].Semergen. 2016 Jul-Aug;42(5):307-14. doi: 10.1016/j.semerg.2014.10.012. Epub 2014 Dec 16. Semergen. 2016. PMID: 25523277 Spanish.
-
Paediatric ultrasonography of the liver, hepatobiliary tract and pancreas.Eur J Radiol. 2014 Sep;83(9):1570-81. doi: 10.1016/j.ejrad.2014.03.025. Epub 2014 Apr 8. Eur J Radiol. 2014. PMID: 24780818 Review.
-
Imaging the pediatric liver: MRI and CT.AJR Am J Roentgenol. 1986 Oct;147(4):785-90. doi: 10.2214/ajr.147.4.785. AJR Am J Roentgenol. 1986. PMID: 3489382
-
Diagnosis of congenital and acquired focal lesions in the neck, abdomen, and pelvis with contrast-enhanced ultrasound: a pictorial essay.Eur J Pediatr. 2018 Oct;177(10):1459-1470. doi: 10.1007/s00431-018-3197-8. Epub 2018 Jul 3. Eur J Pediatr. 2018. PMID: 29971555
Cited by
-
Evaluation of plantar fasciopathy shear wave elastography: a comparison between patients and healthy subjects.J Ultrasound. 2021 Dec;24(4):417-422. doi: 10.1007/s40477-020-00474-7. Epub 2020 May 16. J Ultrasound. 2021. PMID: 32418168 Free PMC article.
-
Ultrasound findings in paediatric cholestasis: how to image the patient and what to look for.J Ultrasound. 2020 Mar;23(1):1-12. doi: 10.1007/s40477-019-00362-9. Epub 2019 Feb 12. J Ultrasound. 2020. PMID: 30756259 Free PMC article. Review.
-
Efficacy of Ultrasound for the Detection of Possible Fatty Liver Disease in Children.Diagnostics (Basel). 2024 Jul 31;14(15):1652. doi: 10.3390/diagnostics14151652. Diagnostics (Basel). 2024. PMID: 39125528 Free PMC article.
-
Risk Factors, Diagnosis, and Treatment of Neonatal Fungal Liver Abscess: A Systematic Review of the Literature.Life (Basel). 2023 Jan 6;13(1):167. doi: 10.3390/life13010167. Life (Basel). 2023. PMID: 36676116 Free PMC article. Review.
-
Liver magnetic resonance elastography and fat fraction in pediatric patients with cystic fibrosis versus healthy children.Pediatr Radiol. 2024 Feb;54(2):250-259. doi: 10.1007/s00247-023-05832-1. Epub 2023 Dec 22. Pediatr Radiol. 2024. PMID: 38133654
References
-
- De Bruyn R (2005) The liver, spleen and pancreas. In: Pediatric US How, Why and When. Elsevier, 131–154
-
- Riccabona M (2013) Liver and Bile System. In: Pediatric US, ed. Springer 213–245
-
- Lafortune M, Madore F, Patriquin H, Breton G. Segmental anatomy of the liver: a sonographic approach to the Couinaud nomenclature. Radiology. 1991;181:443–448. - PubMed
-
- Niederau C, Sonnenberg A, Müller JE, Erckenbrecht JF, Scholten T, Fritsch WP. Sonographic measurements of the normal liver, spleen, pancreas, and portal vein. Radiology. 1983;149:537–540. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
