

Review
doi: 10.1007/s40477-019-00357-6.
Epub 2019 Feb 18.
Neonatal and pediatric thoracic ultrasonography
Affiliations
- PMID: 30778892
- PMCID: PMC6531530
- DOI: 10.1007/s40477-019-00357-6
Item in Clipboard
Review
Neonatal and pediatric thoracic ultrasonography
J Ultrasound.
2019 Jun.
Abstract
Ultrasound examination of the thorax (TUS) can be quite suitable for children because their unique thoracic anatomy provides many acoustic windows into the chest. This review article covers techniques, indications, and applications of TUS in neonates, infants, and children, including common aspects and applications, like pulmonary consolidation and atelectasis, pleural effusion and pneumothorax and main neonatal pathologies such as respiratory distress syndrome (RDS) and transitory tachypnea of the newborn (TTN).
Keywords: Artifact; Chest; Lung disease; Ultrasound.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting in an adult (a) and healthy newborn (b). In b, there is a better anatomical definition of the pleural reflection (hand index finger), with evidence of multiple horizontal reverberation artifacts or A-lines (orange arrows) with some ring-down or B-lines (red arrows) intersecting the above A-lines

Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting in a healthy newborn: the horizontal reverberation artifact, or A-line, in a normal lung surface (green arrow) is parallel to the hyperechoic “pleural line”, which is equidistant (1 2 3 4)

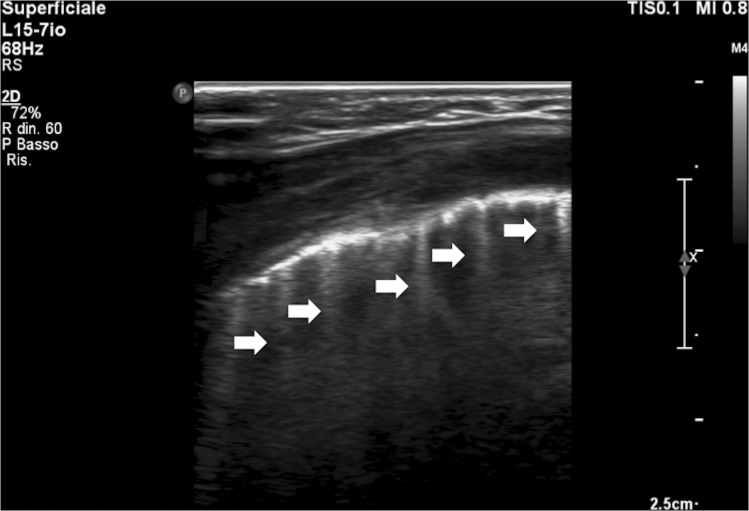
Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting: multiple hyperechogenic linear structures or ring-down artifacts come from the hyperechoic pleural line (white arrow) progress caudally for several cm (orange arrows)
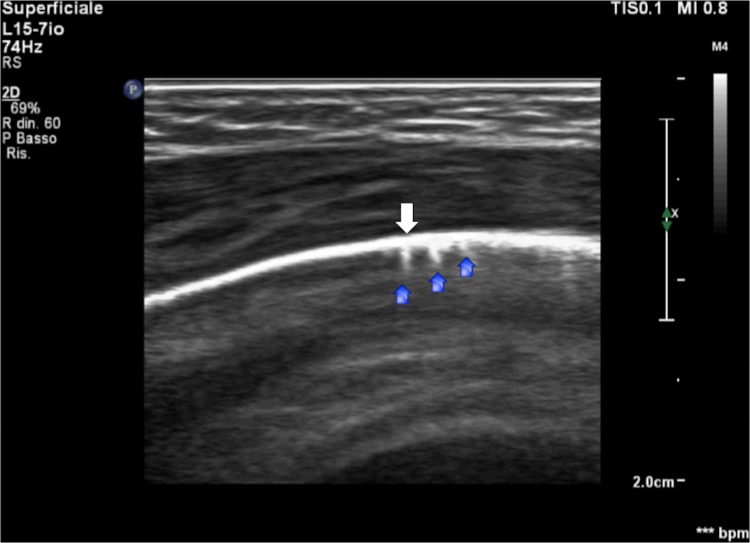
Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting: small linear hyperechogenic artifacts come from the “pleural line” (white arrow) and progress caudally for a few mm as a comet tail (blue arrows)
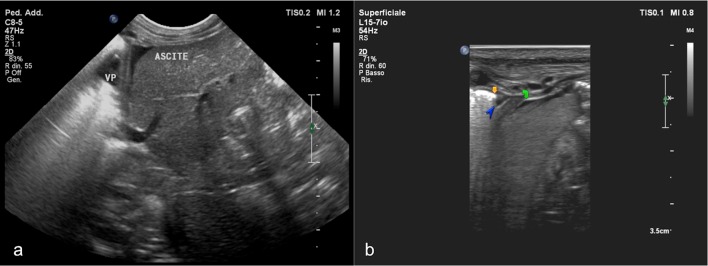
Epigastric longitudinal scan with a micro-convex transducer (8–5 MHz) and pulmonary setting, a clear detection of the hepatic left lobe with visibility of the diaphragmatic interface (white arrow) that separates the thoracic compartment with the minimal fluid component of pleural effusion (VP) and a few sub-diaphragmatic peri-hepatic fluid components referable to ascites. Epigastric longitudinal scan with a high-frequency linear transducer (15–7 MHz) and pulmonary setting, b clear detection of the hepatic left lobe with an excellent view of the diaphragmatic interface that separates the thoracic compartment with minimal fluid components of pleural effusion (blue arrowhead), pulmonary air, outlined by the presence of the pleural line in the extreme front costo-diaphragmatic recess (orange arrow), and few sub-diaphragmatic peri-hepatic fluid components referable to ascites (green arrow)

Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting: small-sized bronchopneumonia (calliper) with blurring of the margins and subtle and irregular hypoechoic appearance that reaches the pleural line, deleting part of the normal pleural hyperechogenicity
Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting in patient with clinical and radiological regression (15 days away) of bronchiolitis virus infections: multiple ring-down artifacts (white arrows) on the middle and posterior axillary right line scans
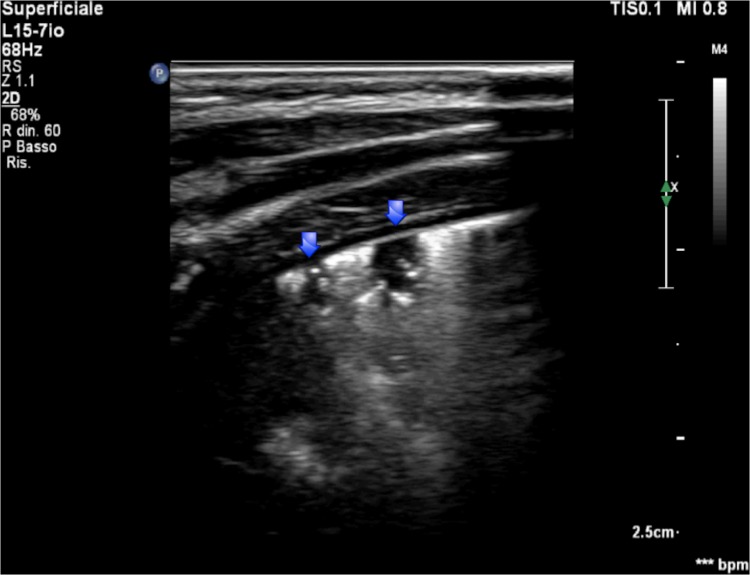
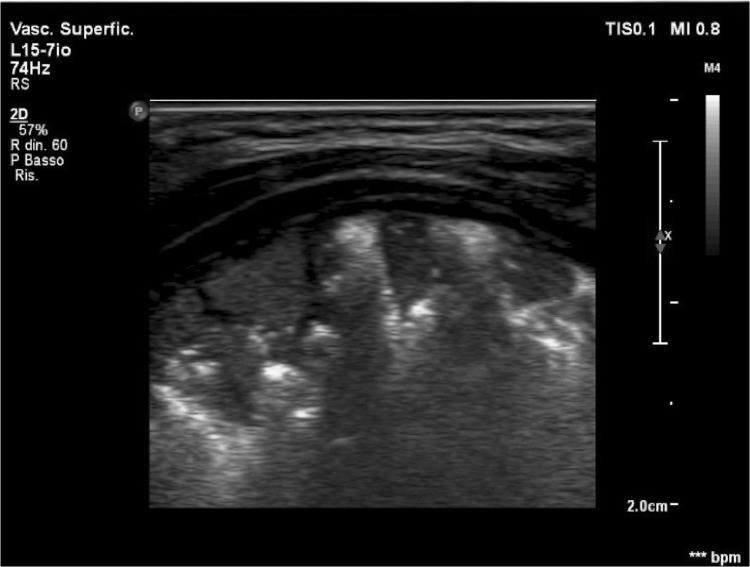
Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting in patients with Down syndrome, inter-atrial defects, and perinatal asphyxia: geometric areas with irregular margins and some hyperechoic spots in the context (blue arrows) on the posterior axillary anatomical right site scans
Chest ultrasound examination performed with a high-frequency linear transducer (15–7 MHz) and pulmonary setting in a distressed newborn: a high number of ring-downs in confluence
Similar articles
-
Potential of ultrasound in the pediatric chest.Eur J Radiol. 2014 Sep;83(9):1507-18. doi: 10.1016/j.ejrad.2014.04.011. Epub 2014 Apr 26. Eur J Radiol. 2014. PMID: 24844730 Review.
-
Role of chest ultrasound in neonatal lung disease: a review of current evidences.J Matern Fetal Neonatal Med. 2019 Jan;32(2):310-316. doi: 10.1080/14767058.2017.1376317. Epub 2017 Sep 14. J Matern Fetal Neonatal Med. 2019. PMID: 28870125 Review.
-
[Lung ultrasonography for the diagnosis of neonatal respiratory distress syndrome: a pilot study].Zhonghua Er Ke Za Zhi. 2013 Mar;51(3):205-10. Zhonghua Er Ke Za Zhi. 2013. PMID: 23751583 Chinese.
-
The 'double lung point': an ultrasound sign diagnostic of transient tachypnea of the newborn.Neonatology. 2007;91(3):203-9. doi: 10.1159/000097454. Epub 2006 Dec 6. Neonatology. 2007. PMID: 17377407
-
Routine application of lung ultrasonography in the neonatal intensive care unit.Medicine (Baltimore). 2017 Jan;96(2):e5826. doi: 10.1097/MD.0000000000005826. Medicine (Baltimore). 2017. PMID: 28079811 Free PMC article.
Cited by
-
Point-of-Care Lung Ultrasound in the Intensive Care Unit-The Dark Side of Radiology: Where Do We Stand?J Pers Med. 2023 Oct 26;13(11):1541. doi: 10.3390/jpm13111541. J Pers Med. 2023. PMID: 38003856 Free PMC article. Review.
-
From an abdominal ultrasound to a lung disease passing through the diaphragm: a case of idiopathic pulmonary fibrosis.J Ultrasound. 2020 Dec;23(4):607-611. doi: 10.1007/s40477-020-00445-y. Epub 2020 Mar 11. J Ultrasound. 2020. PMID: 32162155 Free PMC article.
-
The lung ultrasound: facts or artifacts? In the era of COVID-19 outbreak.Radiol Med. 2020 Aug;125(8):738-753. doi: 10.1007/s11547-020-01236-5. Epub 2020 Jun 13. Radiol Med. 2020. PMID: 32535787 Free PMC article. Review.
-
Relationship between neonatal respiratory distress syndrome pulmonary ultrasonography and respiratory distress score, oxygenation index, and chest radiography grading.World J Clin Cases. 2024 Jul 16;12(20):4154-4165. doi: 10.12998/wjcc.v12.i20.4154. World J Clin Cases. 2024. PMID: 39015913 Free PMC article.
-
Not all abolished lung sliding are pneumothorax: the case of a particular lung atelectasis.J Ultrasound. 2021 Dec;24(4):519-523. doi: 10.1007/s40477-020-00427-0. Epub 2020 Jan 22. J Ultrasound. 2021. PMID: 31970716 Free PMC article.
References
-
- Amin VR (1989) Ultrasonic attenuation estimation for tissue characterization" Retrospective Theses and Dissertations. 17318. https://lib.dr.iastate.edu/rtd/17318
-
- Tole NM (2005) Basic physics of ultrasonographic imaging. Harald Ostensen (ed) Diagnostic Imaging and Laboratory Technology Essential Health Technologies Health Technology and Pharmaceuticals WORLD HEALTH ORGANIZATION Geneva
-
- Cardenas-Garcia J, Mayo PH, Folch E. Ultrasonographic evaluation of the Pleura. Sage J. 2015
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
