

Ultrasonographic and multimodal imaging of pediatric genital female diseases
- PMID: 30778893
- PMCID: PMC6704207
- DOI: 10.1007/s40477-019-00358-5
Ultrasonographic and multimodal imaging of pediatric genital female diseases
Abstract
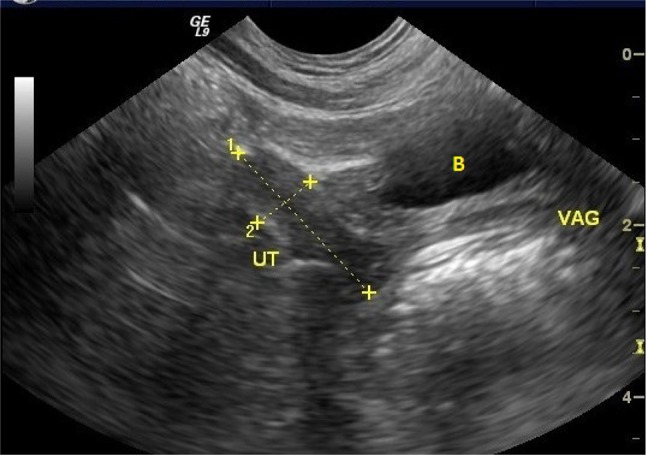
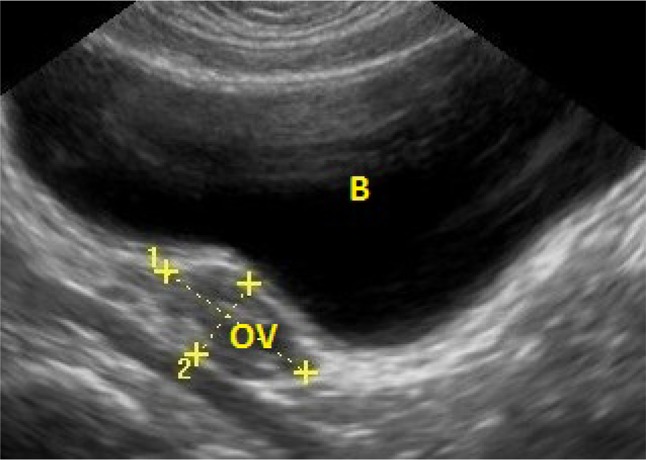
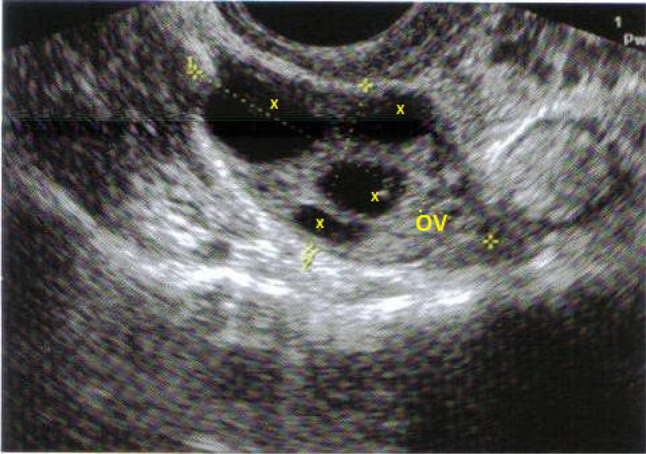
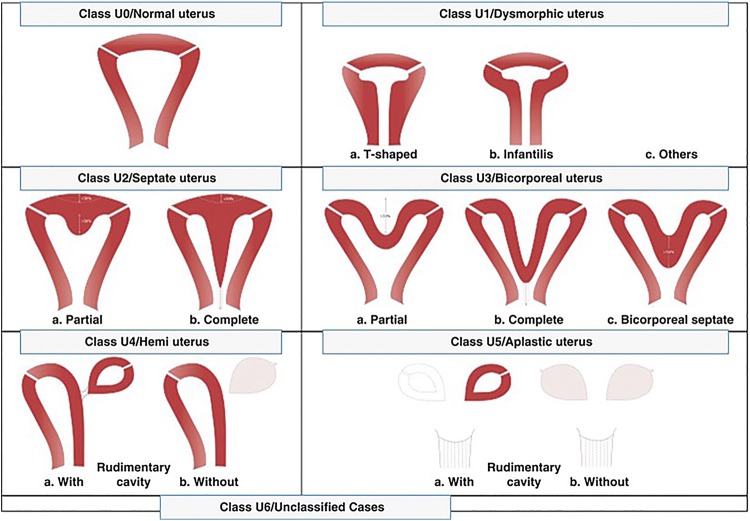
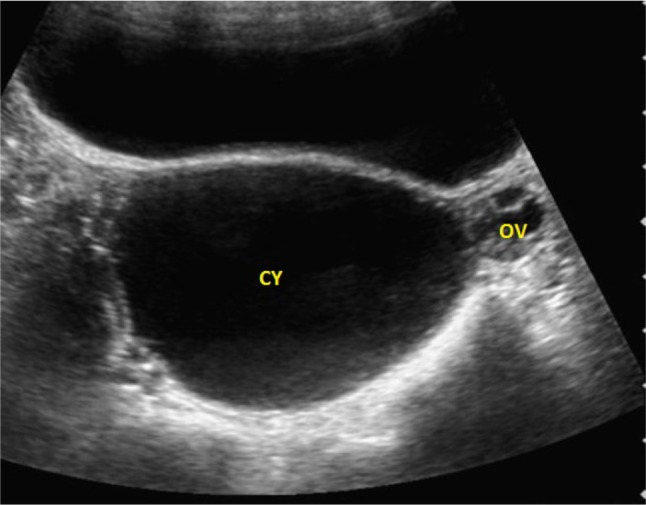
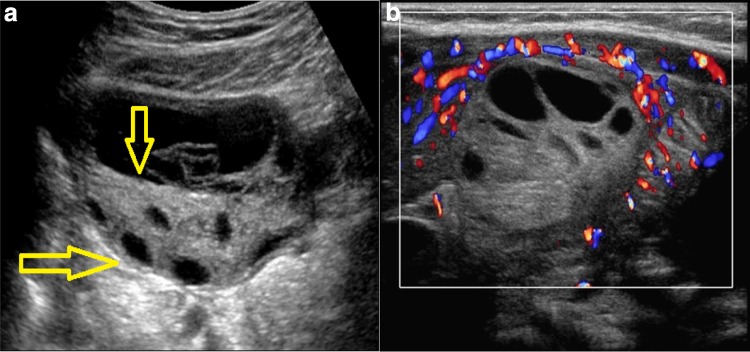
Ultrasonography is the first-line imaging modality in the evaluation of the female pelvis in childhood and adolescence, because it is easy to perform, non-invasive and it does not require sedation. The transabdominal approach is preferred in children and adolescents, after filling the bladder to move away the bowel loops from the pelvis. The probe frequency must be adapted to age, thickness of tissues and depth of the structures under examination. High-frequency (4-12 MHz) linear or convex probes are used in newborns; high-frequency linear probes (4-12 MHz) in toddler, convex 5-7.5 MHz probes in girls and convex 3.5-5 MHz probes in teenagers. In this article, the main pathological conditions of the genital female tract in pediatric age are examined, such as congenital anomalies, disorders of sex development, ovarian cysts, ovarian tumors, adnexal torsion, primary amenorrhea, precocious puberty and pelvic inflammatory disease.
Keywords: Congenital anomalies; Disorders of sex development; Genital female tract; Pediatric age; Pelvic expansive masses; Ultrasound examination.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures





Similar articles
-
Sonographic imaging of the paediatric female pelvis.Eur Radiol. 2005 Jul;15(7):1296-309. doi: 10.1007/s00330-005-2648-6. Epub 2005 Mar 9. Eur Radiol. 2005. PMID: 15756554
-
Ultrasound of the pediatric female pelvis.Semin Ultrasound CT MR. 2008 Apr;29(2):98-113. doi: 10.1053/j.sult.2007.12.002. Semin Ultrasound CT MR. 2008. PMID: 18450135 Review.
-
US of the pediatric female pelvis.Radiology. 2014 Mar;270(3):644-57. doi: 10.1148/radiol.13121724. Radiology. 2014. PMID: 24568702 Review.
-
Ultrasonography of the female pelvis in childhood and adolescence.Radiol Clin North Am. 1992 Jul;30(4):743-58. Radiol Clin North Am. 1992. PMID: 1631281 Review.
-
US of the pediatric female pelvis: a clinical perspective.Radiographics. 2001 Nov-Dec;21(6):1393-407. doi: 10.1148/radiographics.21.6.g01nv041393. Radiographics. 2001. PMID: 11706212 Review.
Cited by
-
Pelvic Pain in Reproductive Age: US Findings.Diagnostics (Basel). 2022 Apr 9;12(4):939. doi: 10.3390/diagnostics12040939. Diagnostics (Basel). 2022. PMID: 35453987 Free PMC article. Review.
-
Skene's glands abscess an overlooked diagnosis in acute lower urinary symptoms.Radiol Case Rep. 2021 Oct 2;16(12):3751-3756. doi: 10.1016/j.radcr.2021.09.006. eCollection 2021 Dec. Radiol Case Rep. 2021. PMID: 34630812 Free PMC article.
-
The role of pelvic ultrasound for the diagnosis and management of central precocious puberty: An update.Acta Biomed. 2021 Nov 4;92(5):e2021480. doi: 10.23750/abm.v92i5.12295. Acta Biomed. 2021. PMID: 34738554 Free PMC article.
-
Pelvic ultrasound and pubertal attainment in girls with sexual precocity: the pivotal role of uterine volume in predicting the timing of menarche.Front Endocrinol (Lausanne). 2024 Jun 25;15:1417281. doi: 10.3389/fendo.2024.1417281. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38989002 Free PMC article.
-
The Evaluation, Diagnosis, and Management of Ovarian Cysts, Masses, and Their Complications in Fetuses, Infants, Children, and Adolescents.Healthcare (Basel). 2025 Mar 31;13(7):775. doi: 10.3390/healthcare13070775. Healthcare (Basel). 2025. PMID: 40218072 Free PMC article. Review.
References
-
- Busilacchi P, Rapaccini GR et al (2006) Ecografia Clinica. Idelson Casa Editrice
-
- Siegel MJ. Pediatric sonography. Philadelphia: Lippincott Williams and Wilkins; 2011.
-
- Beek E, Van Rijn RR. Diagnostic pediatric ultrasound. New York: Thieme; 2016.
-
- Paltiel HJ, Phelps A. US of the pediatric female pelvis. Radiology. 2014;270(3):644–657. - PubMed
-
- Garel L, Dubois J, Grignon A, Filiatrault D, Van Vliet G. US of the pediatric female pelvis: a clinical perspective. Radiographics. 2001;21(6):1393–1407. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
