

ED Door-to-Antibiotic Time and Long-term Mortality in Sepsis
- PMID: 30779916
- PMCID: PMC6533450
- DOI: 10.1016/j.chest.2019.02.008
ED Door-to-Antibiotic Time and Long-term Mortality in Sepsis
Abstract
Background: The impact of antibiotic timing on sepsis outcomes remains controversial due to conflicting results from previous studies.
Objectives: This study investigated the association of door-to-antibiotic time with long-term mortality in ED patients with sepsis.
Methods: This retrospective cohort study included nontrauma adult ED patients with clinical sepsis admitted to four hospitals from 2013 to 2017. Only patients' first eligible encounter was included. Multivariable logistic regression was used to measure the adjusted association between door-to-antibiotic time and 1-year mortality. Secondary analyses used alternative antibiotic timing measures (antibiotic initiation within 1 or 3 h and separate comparison of antibiotic exposure at each hour up to hour 6), alternative outcomes (hospital, 30-day, and 90-day mortality), and alternative statistical methods to mitigate indication bias.
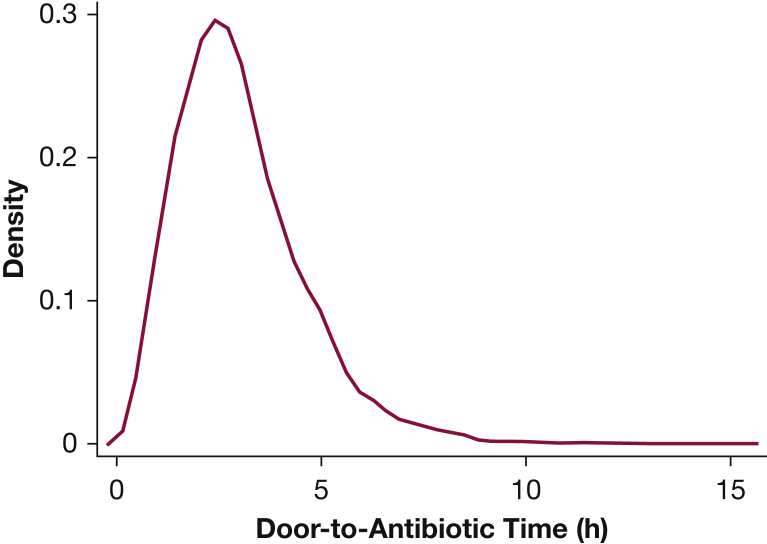
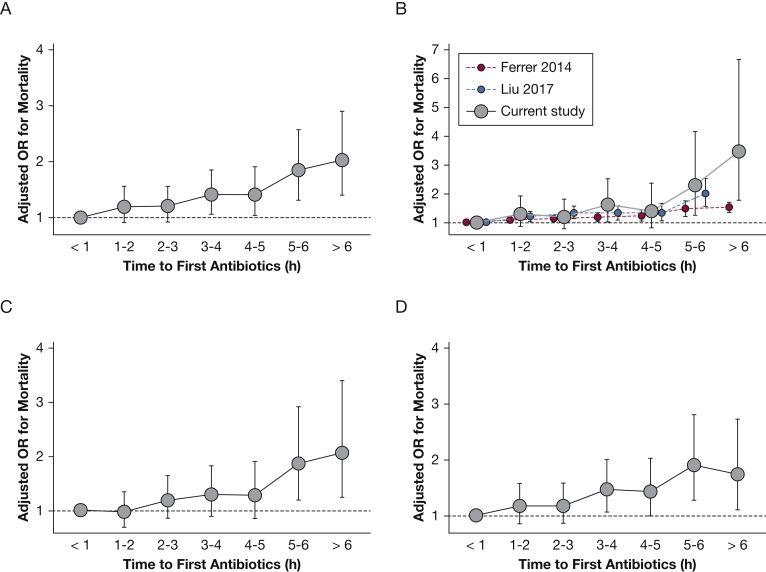
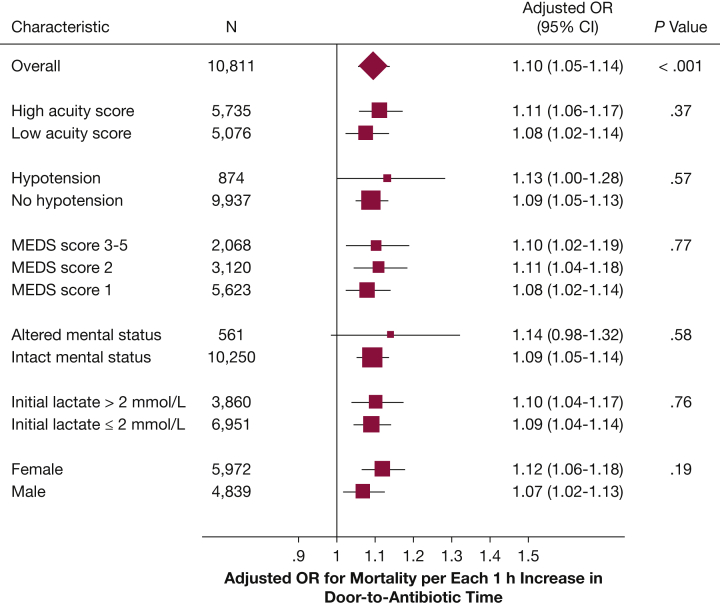
Results: Among 10,811 eligible patients, median door-to-antibiotic time was 166 min (interquartile range, 115-230 min), and 1-year mortality was 19%. After adjustment, each additional hour from ED arrival to antibiotic initiation was associated with a 10% (95% CI, 5-14; P < .001) increased odds of 1-year mortality. The association remained linear when each 1-h interval of door-to-antibiotic time was independently compared with door-to-antibiotic time ≤ 1 h and was similar for hospital, 30-day, and 90-day mortality. Mortality at 1 year was higher when door-to-antibiotic times were > 3 h vs ≤ 3 h (adjusted OR, 1.27; 95% CI, 1.13-1.43) but not > 1 h vs ≤ 1 h (adjusted OR, 1.26; 95% CI, 0.98-1.62).
Conclusions: Delays in ED antibiotic initiation time are associated with clinically important increases in long-term, risk-adjusted sepsis mortality.
Keywords: antibiotic therapy; emergency medicine; epidemiology; mortality; sepsis.
Copyright © 2019 American College of Chest Physicians. All rights reserved.
Figures
References
-
- Vincent J.L. Individual gene expression and personalised medicine in sepsis. Lancet Respir Med. 2016;4(4):242–243. - PubMed
-
- Angus D.C., Barnato A.E., Bell D. A systematic review and meta-analysis of early goal-directed therapy for septic shock: the ARISE, ProCESS and ProMISe Investigators. Intensive Care Med. 2015;41(9):1549–1560. - PubMed
-
- Rhodes A., Evans L.E., Alhazzani W. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45(3):486–552. - PubMed
-
- Levy M.M., Evans L.E., Rhodes A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med. 2018;44(6):925–928. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
